
The use of adhesives to replace traditional invasive internal fixation tools (such as steel plates and nails) will revolutionize orthopedic surgery. The ideal bone cement should be able to immediately fix the fracture site, while providing a space and microenvironment suitable for bone cell growth and promoting fracture healing.
Cyanoacrylate (commonly known as universal glue) is currently the only medical glue with excellent instant adhesive strength and biocompatibility, but its polymerization product is non-degradable and cannot support the growth of new bone tissue through the adhesive layer, which hinders Because of bone healing, it cannot yet be used as a bone cement.
Recently, with the support of the Ministry of Science and Technology, the National Natural Science Foundation of China, and the Chinese Academy of Sciences, Qiu Dong’s group at the has proposed a bioactive glass composite pore-forming strategy to help cyanoacrylate bonding Agents are used for internal fixation of fractures to promote fracture healing. Bioactive glass has excellent osteoconductivity, osteoinduction, and can promote the regeneration of bone tissue.
To prove that the bioactive pore‐forming adhesive is not only strong and instant bonded but also facilitates cell ingrowth and displays excellent bioactivity, they conducted bone‐fracture healing experiments. In the experiment, the bioactive pore‐forming adhesive (PSC1/PEG4/OCA5) was compared with commercial adhesive (OCA) and pore‐forming adhesive (PEG5/OCA5) by applying all to a circular bone piece which was fixed within freshly formed cranial fractures in a group of mice.
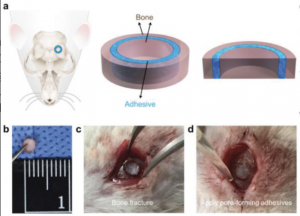
Figure 1. The scheme of a mouse cranial fracture with the craniotomy location (Source)
The stability of the circular bone piece and bone healing effect were evaluated at 12 weeks post‐operation. The ratio of bone volume (BV) within the circular gap over the total volume (TV) within the circular gap was quantified as shown in the figure 2 below. After 12 weeks, BV/TV of the PSC1/PEG4/OCA5 group was 0.76 ± 0.06, which was significantly higher than that of the PEG5/OCA5 group (0.47 ± 0.10), the OCA group (0.40 ± 0.06), and the group with no adhesive treatment (0.26 ± 0.05). These findings supported that the adhesive with pores for bone ingrowth was crucial for new bone formation.
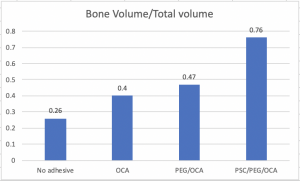
Figure 2. quantitative analysis of new bone formation (Source)
ARS (Alizarin Red S) can detect calcium which is a characteristic evidence to bone‐like structures. As shown in Figure 3, the Ca content in the bioactive pore‐forming adhesive (OD = 0.084 ± 0.008) was around two-fold higher than those in the merely pore‐forming adhesive (OD = 0.046 ± 0.004) and CA adhesive (OD = 0.041 ± 0.001). As a result, these findings were consistent with the statement that the PSC BG can promote osteogenic differentiation that is of importance for bone regeneration.
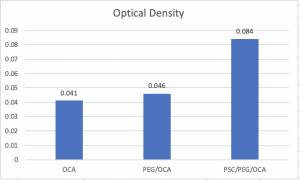
Figure 3. The optical density of eluents from ARS‐stained adhesives (Source)
The bioactive bone cement has good clinical transformation prospects and can provide new ideas and methods for clinical fracture treatment. At the same time, the above-mentioned composite pore-forming strategy can also be used for substances other than bioactive glass to increase matrix materials and functions. Material compatibility.
-Xinyue Yang
Posted on Mar.2nd, 2020