
8 March 2017
For this assignment I reviewed a study conducted by Sarah E. Rogers, Joanne C. Demmler, Rohan Dsilva, Ronan A. Lyons titled Protecting health data privacy while using residence-based environment and demographic data.
The main objective of the authors of this study was to provide a method to link anonymised individual-level demographic data to address-level built environment data. Access to parks and playgrounds (facilities) within 500 meters for children aged 6 to 12 years old by income group was calculated in the city of Swansea, United Kingdom as a worked example of the authors’ anonymisation method.
I was particularly interested in this study because it provided an opportunity to learn more about how sensitive data is anonymised. This is a process that I am not familiar with because all of the data I have worked with is either already anonymised (eg. census data) or do not require to be anonymised. Figure 1 shows the steps the authors took to anonymise the data used for their study.
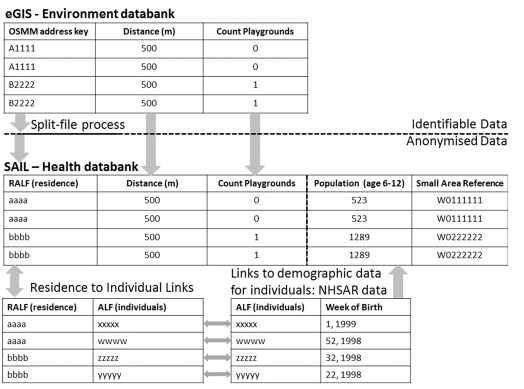
Figure 1. Steps taken to anonymise data for the study. SAIL refers to the Secure Anonymous Information Linkage; RALF stands for Residential Anonymous Linking Field; and ALF stands for Anonymous Linking Field. Figure taken from Demmler et al., 2012)
The anonymised data was then used in an analysis to determine access to parks and playgrounds for each residence with children aged 6 – 12 by household income. The analysis found that children aged 6 – 12 from low income households with has more access to parks or playgrounds than those from high income households. It was also found that income has a larger effect on park and playground access in areas with higher child population densities.
Based on the critiques listed below, I gave the study a 6 out of 10.
- While the study successfully anonymised data for analysis, the process relied heavily on third party organisations such as SAIL and NWIS that charge for their services and as a result may not be feasible for those under a budget.
- I would have appreciated larger discussion of the results of the study eg. What factors cause children in less affluent areas have more access to playgrounds? As well, what are the implications of the results? Are children in less affluent areas less likely to be obese because they have higher access to parks?
- As mentioned in the paper, the study failed to consider the quality of facilities. It is possible that the playgrounds that children of poorer communities are more rundown thereby negating the advantage of having more access to facilities.
References
Demmler, J. C., Dsilva, R., Lyons, R. A., and Rogers S. E. (2012). Protecting health data privacy while using residence-based environment and demographic data. Health and Place. 28, 209 – 217. doi: 10.1016/j.healthplace.2011.09.006
Esri. (2016). Service area analysis. Retrived from http://desktop.arcgis.com/en/arcmap/latest/extensions/network-analyst/service-area.htm