For the second semester of my fourth year, I had my second community rotation at The Orchard, a housing complex that is sustained by the Union Gospel Mission (UGM). Much like my rotation at Broadway Pentecostal Lodge, the goal of the rotation is to provide debridement services as well as health promotion and promoting self-care to individuals in this community. UBC provides three chairs and two dental units for the four UBC dental hygiene students to provide treatment. Clients are recruited by advertising to those who live in the housing complexes, as well as the UGM Welcome Centre.

Calculus removed from a man who has not seen a dental professional for 10+ years.
A stark difference between the two sites, however, is the population that we are serving. UGM provides services for low-income individuals and families, as well as immigrants and refugees. The people who access help from UGM vary greatly in terms of demographics, ethnic and cultural background, and also in terms if their oral health needs. Many of those who sought care at UGM had not seen a dental professional for many years, and some had never seen a dental professional before. It is evident that there is a great need for dental hygiene services within this population, as many people are eager and willing to seek treatment at this community site.
During this rotation, there were many clinical challenges due to the setting that our “clinic” took place, as well as a language barrier between the dental hygiene students and a majority of the clients. However, we were able to provide dental hygiene treatment to a number of individuals in need, and in turn, learned a lot about cultural competency as well as honed our clinical skills in order to provide efficient and effective dental hygiene care.


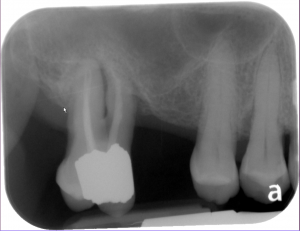 Radiographs revealed generalized horizontal bone loss and areas of vertical bone loss, and mobility in several areas, notably 18.
Radiographs revealed generalized horizontal bone loss and areas of vertical bone loss, and mobility in several areas, notably 18.