The dental hygienist is an important member of the interprofesisonal health team for families. It is important to educate our clients for their own oral health, but also to educate them as a parent for the health of their children’s mouths. In my third year community rotation, my group visited New West Family Place (NWFP). NWFP provides support and resources for families with children up to age 5, and also serves as a drop-in daycare centre where the parents and children can play. NWFP also offers Parent Education Programs, where individuals are invited to speak on several topics, to help educate parents.
We were able to visit NWFP with the goal of raising oral health awareness for the entire family. At this site, we created lessons aimed at educating parents or caregivers of children under five years old. Our topics included nutrition and its impact on oral health, how to access dental services and when it is appropriate to do so for children, and lastly, oral self-care for all family members. We emphasized many issues that parents with young children may face, including baby bottle rot and early childhood caries, teething, as well as any questions that these parents had for dental professionals.
The experience was eye-opening, as I had not previously worked with a family as my “client”. It is important to realize that a client is not always one individual, and to recognize the impact of educating a parent for their own oral health, and for their children. We learned that raising oral health awareness and knowledge of one family member has the potential to improve the oral health of the entire family.

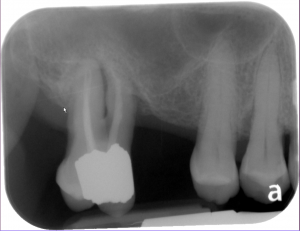 Radiographs revealed generalized horizontal bone loss and areas of vertical bone loss, and mobility in several areas, notably 18.
Radiographs revealed generalized horizontal bone loss and areas of vertical bone loss, and mobility in several areas, notably 18.