The assessment protocol for RAD is one of unique nature. RAD is one of the few diagnoses in the DSM-V where very little is known about the disorder, so a valid, universal assessment protocol has yet to be established. This lack a universal assessment protocol, along with the lack of knowledge regarding RAD, has led to 3 overarching problems.

Three General Issues with Assessment for RAD:
- There is a lack of assessment tools that are made specifically for RAD
- There is no consensus amongst the research community regarding which assessment tools are most valid to use when assessing for RAD
- Confusion with other disorders vs. RAD
It is very problematic that there are limited resources and tools to assess for RAD. RAD is already a difficult diagnosis to make with it being rare and having subtle symptoms that are easily missed, and the lack of resources adds to the difficulty for practitioners to identify children with RAD. Assessment is a key piece to putting the puzzle of RAD together, and any diagnosis for that matter, because an official diagnosis helps identify and offers some answers to the problems that are occurring for a child, it helps guide treatment plans and assists in obtaining any funding. It is critical that the research community works to establish a universally, accepted assessment protocol for RAD so that practitioners and clinicians are confident when assessing and diagnosing this disorder.

Potential Assessment Tools for RAD:
There are several assessment tools that are applicable when assessing RAD. However, it is crucial to note that these assessments were not made specifically for RAD; they were created to identify other diagnoses. These assessments may be utilized because they observe similar behaviors and presentation of symptoms as RAD, but the validity of these tests for accurately assessing RAD is questionable.
In general, these tools aim to assess these three components of the child and their life:
- The child’s patterns of attachment:
- Attachment is the primary component when diagnosing RAD, as it is a diagnosis based on whether the child has developed healthy attachments to their parents/caregivers or not. For RAD, clinicians would be specifically looking for a lack of attachment.
- Attachment assessments are intended to cover the spectrum of attachment-related behaviors, such as:
- Whether the child has a secure, avoidant, ambivalent, or disorganized attachment
- Healthy exploratory behaviors
- Emotional withdrawal/inhibited from caregiver
- Self-protective behaviors
- If they identify caregiver as a source of danger or protection
- Affective responses and social cognition
- Examples of attachment assessments:
- The Strange Situation Procedure (SSP)
- Preschool Assessment of Attachment
- Disturbances of Attachment Interview (DAI)
2. Children’s representations of relationships:
- Children with RAD are presumed to have grossly disturbed internal working models of relationships that may lead to interpersonal and behavioral difficulties in later life.
- By analyzing children’s mental representations of relationships gives us another glimpse into understanding what type of relationships/attachment they consider typical and the type of relationships they have been exposed to as well.
- To identify children’s representations of relationships, practitioners may:
- Ask about the child’s memories and perceptions of their caregivers
- May conduct role-play with puppets
- May conduct “what happens next” scenario tests where the child finishes a scenario about relationship interactions.
- Examples of attachment assessments:
- MacArthur Story Stem Battery
- Story Stem Assessment Profile
- Child Attachment Interview
3. The child’s behavioral, psychological and emotional attributes
- For a RAD diagnosis, clinicians (psychiatrist, psychologist, doctor, mental health professional) would be looking for signs such as:
- A lack of social approach where they fail to initiate or respond to social interaction in developmentally appropriate ways
- Unexplained withdrawal, fear, sadness, or irritability by others
- Sad and listless appearance
- Failure to smile
- Frozen watchfulness
- Not seeking comfort or no response when comfort is given
- Failing to ask for support or help
- Failure to reach out when being picked up
- No interest in social interaction with interactive games
- Oversociable
- Fail to show selective attachments
- Demonstrate clinging and/or indiscriminate friendliness, even in their interactions with strangers
- Examples of attachment assessments:
- The Strengths and Difficulties Questionnaire (SDQ)
- Behavioural Assessment System for Children (BASC)
Additional Potential Assessments for RAD:

Sheperis, C. J., Doggett, R. A., Hoda, N. E., Blanchard, T., Renfro-Michel, E. L., Holdiness, S. H., & Schlagheck, R. (2003). The development of an assessment protocol for reactive attachment disorder. Journal of Mental Health Counseling, 25(4), 291-310.
Assessment tools created for RAD:
Unfortunately, RAD only has 3 assessment tools that were specifically designed to identify the disorder. This severely limits clinicians on the types of methods they may utilize to identify RAD, confidently knowing that the assessments they administer are valid for RAD. However, since there are much debate and division amongst the researcher community and clinicians on the characteristics of RAD, much of the disorder is suspected to be unknown, and these 3 tools are fairly new, many question the validity and reliability of the tools that were designed with for RAD.
There are two questionnaires:

- The Relationship Problems Questionnaire & The Reactive Attachment Disorder Questionnaire
- Both aim to assess and screen symptoms of the inhibited and disinhibited subtypes ofRAD
Parents, guardians, foster parents, and teachers are able to answer these questionnaires- There is little published pertaining to the reliability and validity of these measures
- Rating of Inhibited Attachment Behaviour Scale (RInAB)
- The only observant behaviour screening measure of RAD
- Made for preschool years
- It is based on attachment theory and the DSM 5. Analyzes attachment behaviour, exploratory behaviour, and socioemotional behaviour
- Only created a few years ago
- Internal validity & reliability may be questionable
Confusion between RAD & other disorders:
Many symptoms of RAD overlap with other disorders and are often comorbid with or confused with RAD. This complicates assessment, and it is critical for clinicians to rule out any other disorder that may explain the child’s symptoms before finalizing the diagnosis of RAD.
Some diagnosis that RAD is confused with include:



Recommended steps when suspecting a diagnosis of RAD:
- Educate yourself
- Educators, parents, foster care parents, social workers (etc.) would not be making the official diagnosis of RAD; however, it is important that we are knowledgeable and understand RAD, recognize signs for RAD and so forth in order to understand how to best support children with this diagnosis and make an informed decision regarding pursuing further assessment and which treatment path(s) should be taken.
- Gather as much information as you can about the child’s family history and home environment
- History of current and past living environments
- Who is the child’s current caregiver
- If the child has been adopted or institutionalized, in foster care or lives with their birth parents
- Any patterns of abuse, violence, neglect, and/or abandonment
- Any parental addictions, mental illness in the family, parental incarceration
- Poor living environments and/or low social economic standing
- Gather information about the child:
- Observed behaviour (both good & concerning behaviour)
- The child’s emotional attributes and responsiveness
- Their social skills and/or lack of responding
- Any suspected or diagnosed mental health issues
- Cognitive and language skills/deficits
- Suspected attachment styles
- It is very important to gather as much information as you can about the child’s history because this history is a critical component in establishing developmental timelines for the onset and duration of the symptomology of RAD, which greatly effects the final diagnosis.
- Refer to a medical professional (doctor/psychologist/psychiatrist) who has the credentials and experience in child development and differential diagnosis to further observe and properly assess for RAD
- Clinicians assessing children with RAD should ideally be multifaceted approach using various assessment methods and tools, such as: semi-structured interviews, attachment-specific scales, psychological evaluations, and behavioural observations. Clinicians should use the information from their assessments, along with the information regarding the child’s personal, medical, and family history to make the final diagnosis of RAD.
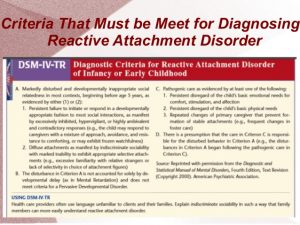
To meet the diagnosis of RAD, this criteria must be relevant in the child’s life:
- Abuse (physical, sexual, and/or psychological), in addition to neglect
- Associated emotional disturbance
- Poor social interaction with peers, poor or lack of interpersonal relationships, social withdrawal, aggression towards self and others, misery, and growth failure in some cases
References:
Golden, J. A. (2009). Introduction to a special issue on the assessment of children with reactive attachment disorder and the treatment of children with attachment difficulties or a history of maltreatment and/or foster care. Behavioral Development Bulletin, 15(1), 1-3.
Hornor, Gail, RNC, MS, CPNP. (2008). Reactive attachment disorder. Journal of Pediatric Health Care, 22(4), 234-239.
Bruce, M., Young, D., Turnbull, S., Rooksby, M., Chadwick, G., Oates, C., Nelson, R., Young-Southward, G., Haig, C., & Minnis, H. (2018). Reactive Attachment Disorder in maltreated young children in foster care. Attachment & Human Development. 1-18.
Sheperis, C. J., Doggett, R. A., Hoda, N. E., Blanchard, T., Renfro-Michel, E. L., Holdiness, S. H., & Schlagheck, R. (2003). The development of an assessment protocol for reactive attachment disorder. Journal of Mental Health Counseling, 25(4), 291-310.
Vervoort, E., De Schipper, J. C., Bosmans, G., & Verschueren, K. (2013). Screening symptoms of reactive attachment disorder: Evidence for measurement invariance and convergent validity. International Journal of Methods in Psychiatric Research, 22(3), 256-265.