Read the article here.
Flexible Learning in Nursing
By Michael Wong on June 30, 2015
As part of the flexible learning initiative, the UBC School of Nursing is implementing a hybrid approach to course delivery in the undergraduate curriculum. The hybrid approach links theoretical concepts and practice competencies by using a mixture of online content, in-class activities, and clinical practice. For Associate Professor Maura Macphee, one of the goals of the flexible learning approach has been to “operationalize the theory” in the clinical setting. “We created a hybrid model of education,” notes Maura. “Whatever we did online, [we wanted to] link it to classroom activities.”
The Bachelor of Science in Nursing is a 20 month accelerated undergraduate program, with 120 students per cohort. “Our program is the shortest in Canada,” states Maura. At the 2015 CTLT Spring Institute, Maura was joined by colleagues from the School of Nursing to share their experience and discuss how the hybrid approach is enhancing student learning, engagement, and satisfaction.
Ranjit Dhari and Joanne Ricci are the instructors for NURS 336: Professional Nursing Practice with Communities and Populations. They transformed their six-week course by using the flipped classroom approach.
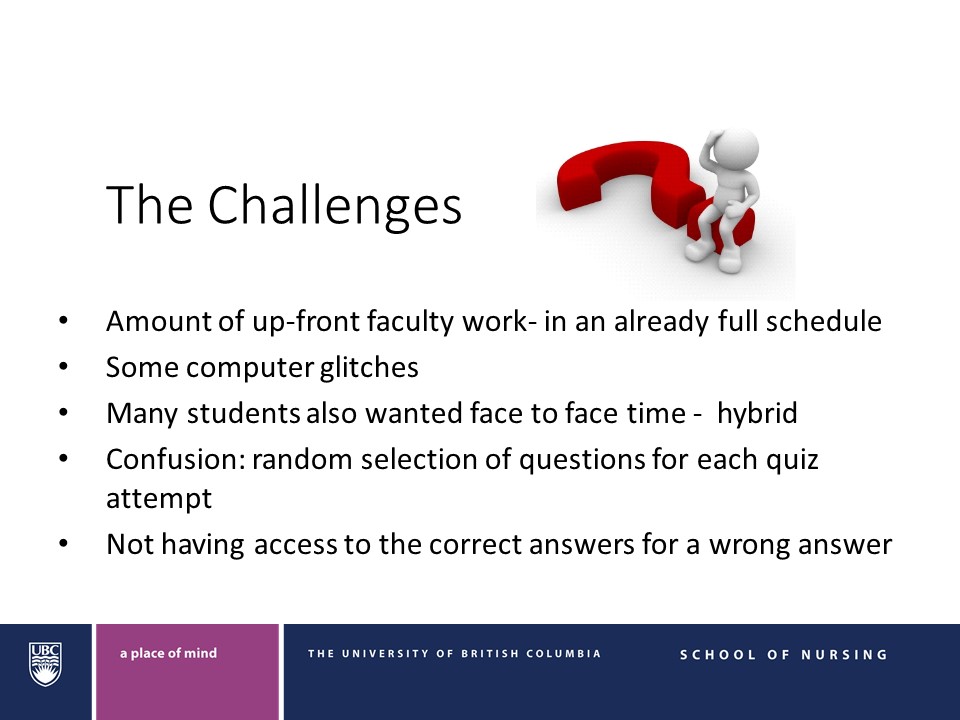
In NURS 336, Ranjit and Joanne invite a number of guest speakers, who work in the profession, to share their expertise with the students. This provides a key link between the theory and clinical practice. However, Ranjit and Joanne have faced a number of challenges with bringing in guest speakers. “These experts are hard to get on a consistent basis,” explains Joanne. “When we would phone our partners in the community to be a guest speaker, they could help out maybe one or two times per year.” Unfortunately, this means that the same guest speakers are not available for each course offering. This adds some content variability across each six-week course.
Another challenge has been to make the content of the guest speakers available to all students. One solution has been to video tape the experts. “We decided to do a video. To video tape our guest speakers,” notes Ranjit. The guest speakers were videotaped in the Applied Science studio space, and Learning Technology Rovers helped edit the videos. The final videos were then uploaded to the Connect course site for all students to view.
After consulting the Centre for Teaching, Learning and Technology (CTLT) about the instructional design of the course, Ranjit and Joanne decided to shorten the length of the guest speaker videos. Ranjit notes that they were advised that students would not watch such a long video. “We looked at converting the one hour talking head and chunked it up,” she says. Ranjit and Joanne worked with the Learning Technology Rovers to edit the videos into shorter, more digestible segments, and organized the videos into the relevant population-based sections of the course.
At the end of each video, Ranjit and Joanne included embedded questions and recommendations. “We embed questions in their learning…so they can use this knowledge in the arena of public health,” says Joanne. “We looked at how can we make it interactive,” adds Ranjit.
Both Ranjit and Joanne acknowledged that the rapid pace of the course can lead to faculty burnout. “It is exhausting to do it every six weeks,” states Joanne. By having a break with the flipped classroom sessions, faculty are able to spend more time developing the course.
Joanne has also found it advantageous to move some of the in-class lecture time online, so that students can view the information at a time that is convenient for them. “It has been helpful to give them that flexibility,” she states.
Ranjit has noticed that students are making good use of the time that was normally dedicated to face-to-face lectures. She has found that students use the time to email her questions or book office hour appointments. Ranjit has also found that fewer students are needing extra time for their assignments. “I’ve gotten less requests for extensions,” she says.
Cathy Ebbehoj teaches NURS 333: Professional Nursing Practice with Childbearing Individuals and Families. Similar to Joanne and Ranjit, Cathy used a flipped classroom approach with her course.
Cathy developed the infant feeding section of the course into an online module in Connect. She feels that the infant feeding material is important, as students need a strong knowledge base of infant feeding prior to going into a clinical setting. “We intentionally looked at the sub-topics,” she notes. “We wanted to make sure we had a comprehensive view.”
Cathy pointed to the fact that many families want in-depth knowledge about infant feeding. As a result, Cathy would often accompany her PowerPoint slides with additional information. “I would [use] different resources for different students,” explains Cathy. For example, she would often include references to textbooks, YouTube videos, and other website resources in order for students to gain a better understanding of the material.
“Be prepared that there is going to be a fair amount of work,” says Cathy. “We found we had to be really intentional…we had to think in a whole different way.” As a result, Cathy used visuals and embedded videos to enrich the online course content. She also did voice-overs to help supplement some of the PowerPoint slides. “I tried to make sure that we broke it down for the students,” notes Cathy. “At the end of each subtopic, we had an assessment, a quiz…It helped solidify their knowledge.”
Cathy noted that she tries to help students think like a nurse. “The other thing we tried to do was to bring theory to practice,” she says. “We asked students to look at policies…and how they were employed in the hospital.” Cathy also tries to have the students draw on their own expertise and experience in order to bridge some of the gaps between the theory and clinical practice.
The second cohort of students is now using the online module, and Cathy has received positive feedback. “They [said that] the videos and external resources were really helpful,” she says. The content has been useful for students to refer to when they are in the clinical setting, and the added flexibility has been beneficial. “They really liked that they could complete the modules on their own time and at their own pace,” says Cathy. “They felt that they were better prepared to go into clinical.”
Cathy feels that the hybrid learning environment works well for her course. The mixture of face-to-face and online course content provides a good balance for the students. “I think that doing a mix is probably the right thing,” says Cathy. Student feedback indicates that while the students have enjoyed the flexibility of the online course content, they still like the face-to-face component and the ability to ask questions of the instructors.
Cheryl Segaric is the instructor for NURS 303: Introduction to Professional Nursing Practice with Adults, Older Adults, and their Families. There are three components to the eight credit course: theory, clinical practice, and clinical lab work. “The course is very high stakes for the students,” notes Cheryl.
Cheryl’s goal was to replace 12 hours of in-class content with online learning. This involved a lot of upfront work. “The workload was quite substantial initially,” she explains. However, Cheryl has found that the workload is beginning to ease off now that the course is in its third iteration.
For her course, Cheryl finds that the online learning environment allows for more participation, from more students. “With flexible learning, everyone gets to participate,” she states. “Everyone has to contribute.” Cheryl finds that with 120 students, not all of them can talk or participate in an in-class setting. By using online group discussions in Connect, she finds that all students are able to get involved. “It is more active and engaging,” she states. Cheryl has also noticed that the online contributions result in richer discussions, with more breadth and depth than in-class discussions. “It promotes a higher level of thinking,” exclaims Cheryl.
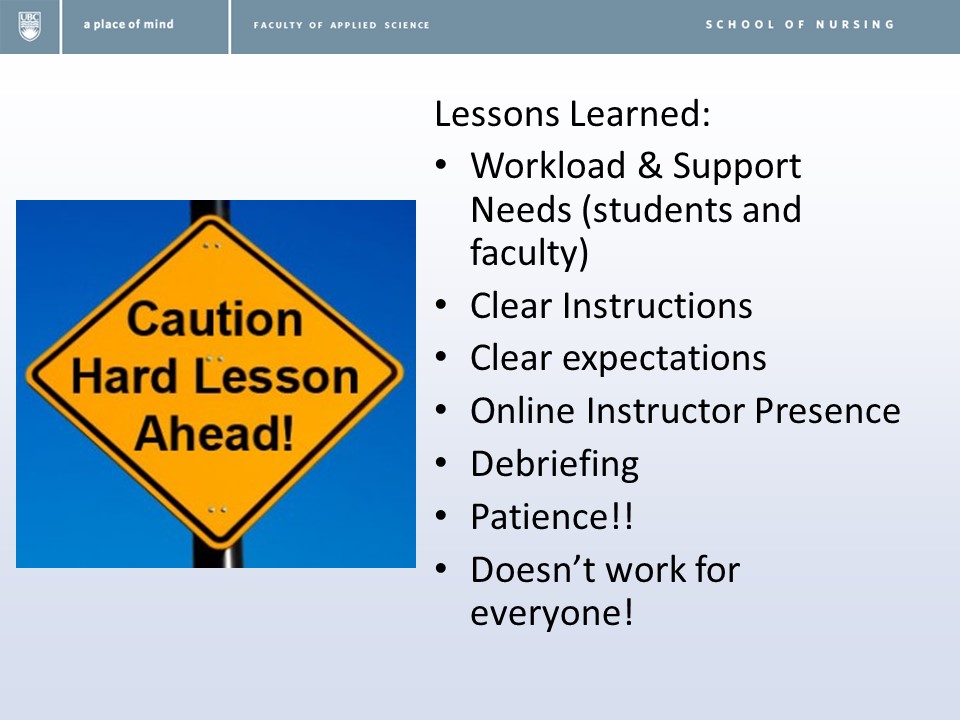
With her experience, Cheryl has found that students require guidance with the group discussions. “It is important to give very clear instructions,” she says. “Be clear about what students should be talking about.” Cheryl also advises other instructors to monitor the discussion boards. “You need to be monitoring those discussions,” she advises, “so they know that you are engaged with them…My TA has really helped with that.”
Students in NURS 303 also use the Canadian Neighbourhood Online Program. The online program includes a number of case studies, photos and medical charts, and patient profiles. It also has videos of conversations between a client and the physician. “It helps them really engage with the content,” states Cheryl. “It sort of personalizes it.” The physician and client interaction videos help students gain both the medical perspective and the client perspective. “It helps create a deeper understanding of the progressions of illness over time,” notes Cheryl.
By incorporating the Canadian Neighbourhood Online Program, Cheryl has noticed that the students are better able to make connections between theory and practice. “I am seeing some evidence that this is working to the benefit of the students,” she notes. With the online module, Cheryl finds that her students are able to break down what is happening, synthesize relevant information, and understand and apply that information to a particular case. “I can start to see that they are actually remembering [information], then moving to a level of understanding,” explains Cheryl. “They are taking the information and applying it to the case.”
All of the instructors expressed that the hybrid learning approach has proved to be very beneficial. “I think we made good progress with the online learning piece and active learning piece,” says Maura. Joanne pointed out that each instructor is implementing flexible learning in slightly different ways. “We are all doing it a little bit differently,” she noted. “It meets our course needs and the students’ needs.” The mixture of face-to-face and online learning has also worked well for Cheryl. “I like the blended [hybrid] learning piece,” she notes. “My take home message…is how valuable it’s been,” adds Cathy.
Maura concluded by acknowledging the collaborative effort that was involved in redesigning the courses. “We couldn’t have done it without support from CTLT, CIS [Centre for Instructional Support in the Faculty of Applied Science], and the LTRs [Learning Technology Rovers],” says Maura. “They were really supportive,” adds Cathy. “We couldn’t have asked for a better team.”

![5IExquw8kT6ULwViQIouvbOW7modmOcaQkRcYaHMe00,9QT-66ek1FN_Fx_cb-zYDQXsqX9z14fZ7-tbxq7sQgQ[1]](https://blogs.ubc.ca/teachingmatters/files/2016/01/5IExquw8kT6ULwViQIouvbOW7modmOcaQkRcYaHMe009QT-66ek1FN_Fx_cb-zYDQXsqX9z14fZ7-tbxq7sQgQ1.jpg)





{kind=link}