Summary
Gay and bisexual men face unique health challenges in the context of social stigma and marginalization. In particular, populations of gay and bisexual men have high rates of HIV and forms of mental distress, including suicidal thoughts and actions.
While new interventions to prevent and treat HIV have substantially decreased the morbidity and mortality associated with the virus, relatively few interventions have been developed to prevent suicide—and even fewer focused on gay and bisexual men as a unique population. To inform and inspire a response to the suicide epidemic among gay and bisexual men, we used an indirect statistical method to estimate mortality attributable to HIV and to suicide, between 1999 and 2017, among gay and bisexual men in the United States (US) and Canada.
Our results were published in the journal Critical Public Health in 2015. Below we provide:
- Updates to our previous analyses, including trends for both the US (data available up to 2017) and Canada (data available up to 2016);
- A description of methods used to generate these estimates; and,
- Links to the data and other resources.
Results
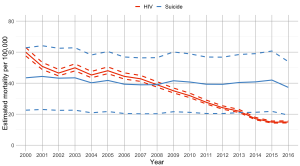
Estimated suicide and HIV-related mortality rates among gay and bisexual men, Canada, 2000–2016 (* see “Data sources” for below for accompanying citations)
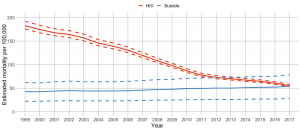
Estimated suicide and HIV-related mortality rates among gay and bisexual men, United States, 1999–2017 (* see “Data sources” for below for accompanying citations)
Methods
What is the population attributable fraction (PAF)?
PAF is a formula used by epidemiologists to estimate the proportion of events (i.e., deaths or other health outcomes) that are attributable to some underlying “exposure”. Traditionally, an exposure is something that causes a disease. We use gay and bisexual sexual orientations not as a traditional exposure but rather as a proxy for a collection of experiences associated with these minority sexual orientations—most especially forms of minority stress that contribute to the elevated rates of suicide among gay and bisexual men.
How does application of the PAF produce mortality estimates?
The PAF is a function of the following two factors:
- pr is the proportion of the total population who are “exposed”, in this case, gay and bisexual men.
- RR, or relative risk, is the relative difference in rates of events between the two groups, in this case gay and bisexual men, and heterosexual men.
More specifically: PAF = [pr(RR – 1)] / [1 + pr(RR – 1)]
For our study, we assumed that 4% of the adult male population are gay or bisexual, i.e., pr=0.04. This is based on surveys from the US and Canada, which suggest that 3-4% of adults outwardly identify as gay or bisexual (e.g., see compiled estimates from The Williams Institute). We then adjust this estimate upward, accounting for the fact that as many as a third of gay and bisexual men will not disclose their sexual orientation in government surveys.
For HIV, we assumed a relative risk (RR) of 42, based on a meta-analysis, that is, statistics compiled from multiple data-sets. We varied this estimate, between 38 and 48, to account for statistical uncertainty in the meta-analysis.
For suicide, we assumed a relative risk (RR) of 3, also based on a meta-analysis. We varied this estimate, between 2 and 4, to account for statistical uncertainty in the meta-analysis.
For each year of analysis, we pulled counts of the number of suicides and HIV-related deaths among adult men, from the US Centers for Disease Control and Statistics Canada websites. We then multiplied these numbers by the PAF for each cause of death to get an annual count of deaths among gay and bisexual men.
Finally, we multiplied Census estimates for the annual population of adult men by 4% to get annual estimates of the population of gay and bisexual men. We estimated mortality rates by dividing the count of deaths among gay and bisexual men by the population of gay and bisexual men.
Why can’t we just directly count the number of deaths among gay and bisexual men?
Sexual orientation data is not currently attached to death certificates in the US or Canada. Some researchers have instead tried to collect sexual orientation information after a death. This approach is not reliable, however, because it requires next of kin to disclose gay or bisexual identities which may not be known to others.
What is the goal of this project?
Our goal in generating these estimates is help public health and community practitioners to prioritize their response to the various causes of premature mortality in communities of gay and bisexual men. For example, in Canada, we have used these results to motivate a network of individuals and organizations who are finding new ways to detect and prevent cases of suicidality in our community. This network includes researchers who have conducted in-depth studies to understand the causes and circumstances of suicide in LGBTQ2 people. It also includes mental health providers who are working to be more LGBTQ2-inclusive and affirming.
Are these estimates accurate?
These estimates depend on several critical assumptions. First, we assume that the population of gay and bisexual men, as a proportion of the adult male population, is fixed over time at 4%. We know, however, that rates of gay and bisexual identity have been increasing over time. Some of this change likely reflects a decrease in negative social attitudes toward gay and bisexual people. We also assume that the relative risk (RR) comparing rates of HIV and suicide attempts between gay/bisexual men and heterosexual men are equivalent to the RR comparing HIV-related deaths and suicides between gay/bisexual and heterosexual men. Verification of these assumptions will require further research, and new methods for measuring sexual orientation in relation to cause-specific mortality. In the meantime, we propose that these indirect estimates be used not as precise estimates but rather as approximate estimates with some margin of error.
Data sources
Canada: Mortality and population count data were adapted from Statistics Canada, CANSIM (1 May 2019). This does not constitute an endorsement by Statistics Canada of this product.
US: United States Department of Health and Human Services (US DHHS), Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Underlying Cause of Death 1999-2017 on CDC WONDER Online Database, released 2018. Data are compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.
Data for year 2017 are compiled from the Multiple Cause of Death File 2017, Series 20, No. 2W, 2018.
Data for year 2016 are compiled from the Multiple Cause of Death File 2016, Series 20, No. 2V, 2017.
Data for year 2015 are compiled from the Multiple Cause of Death File 2015, Series 20, No. 2U, 2016.
Data for year 2014 are compiled from the Multiple Cause of Death File 2014, Series 20, No. 2T, 2015.
Data for year 2013 are compiled from the Multiple Cause of Death File 2013, Series 20, No. 2S, 2014.
Data for year 2012 are compiled from the Multiple Cause of Death File 2012, Series 20, No. 2R, 2014.
Data for year 2011 are compiled from the Multiple Cause of Death File 2011, Series 20, No. 2Q, 2014.
Data for year 2010 are compiled from the Multiple Cause of Death File 2010, Series 20, No. 2P, 2012.
Data for year 2009 are compiled from the Multiple Cause of Death File 2009, Series 20, No. 2O, 2012.
Data for year 2008 are compiled from the Multiple Cause of Death File 2008, Series 20, No. 2N, 2011.
Data for year 2007 are compiled from the Multiple Cause of Death File 2007, Series 20, No. 2M, 2010.
Data for years 2005-2006 are compiled from the Multiple Cause of Death File 2005-2006, Series 20, No. 2L, 2009.
Data for years 1999-2004 are compiled from the Multiple Cause of Death File 1999-2004, Series 20, No. 2J, 2007.
Accessed at http://wonder.cdc.gov/ucd-icd10.html.
Further information
Mortality data can be obtained at the following links.
US Centers for Disease Control and Prevention: https://wonder.cdc.gov/
Statistics Canada: https://www150.statcan.gc.ca/n1/en/type/data
The authors’ full manuscript of the Critical Public Health publication is available here: https://www.cbrc.net/suicide_and_hiv_as_leading_causes_of_death_among_gay_and_bisexual_men
Other references:
Ferlatte O, et al. Disclosure of Sexual Orientation by Gay and Bisexual Men in Government-Administered Probability Surveys. LGBT Health 2017;4(1). https://www.liebertpub.com/doi/10.1089/lgbt.2016.0037
Gates GJ. How many people are lesbian, gay, bisexual, and transgender? The Williams Institute 2011. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf
Plöderl M, et al. Suicide risk and sexual orientation: a critical review. Archives of Sexual Behavior 2013;42(5):715-27. https://www.ncbi.nlm.nih.gov/pubmed/23440560
Purcell DW, et al. Estimating the population size of men who have sex with men in the United States to obtain HIV and syphilis rates. Open AIDS Journal 2012;6:98-107. https://www.ncbi.nlm.nih.gov/pubmed/23049658
Salway T, et al. Evidence of Multiple Mediating Pathways in Associations Between Constructs of Stigma and Self-Reported Suicide Attempts in a Cross-Sectional Study of Gay and Bisexual Men. Archives of Sexual Behavior 2019;47(4):1145-1161. https://www.ncbi.nlm.nih.gov/pubmed/28821997
Salway Hottes t, et al. Lifetime Prevalence of Suicide Attempts Among Sexual Minority Adults by Study Sampling Strategies: A Systematic Review and Meta-Analysis. American Journal of Public Health 2016;106(5):e1-e12. https://ajph.aphapublications.org/doi/10.2105/AJPH.2016.303088
Same-sex couples and sexual orientation… by the numbers. Statistics Canada 2015. https://www.statcan.gc.ca/eng/dai/smr08/2015/smr08_203_2015