As I read through my e-folio, one quote from John Dewey came to mind:
“If we teach today’s students as we taught yesterday’s, we robe them of tomorrow.”
When I started my ETEC 533 journey, I seemed to have been quite disgruntled at the current state of education technology use in the medical school classroom. This was further highlighted in my interview with Dr C, which confirmed that technology was mostly being used to disseminate information that was previously presented by other means. It is a very knowledge-centered, teacher-focused method of teaching. As Cristina Leo pointed out in her Unpacking assumptions post “[digital] technology goes beyond the replacement of an ‘old’ way of doing something, but rather is innovative and modifies and redefines the original task.” This notion was echoed by many of my peers in this class. As I read through the many interviews from module A, I found the contrast between what was happening with education technology in medical school classrooms compared to the many examples of effective use of education technology in K-12 classrooms striking. Reflecting on my blogs entries, I notice that this contrast had me running to excuses for why my colleagues and I have failed to use education technology effectively in our classrooms. For example, I noted that we had many barriers, such as large classroom sizes, lack of training and lack of time. These barriers were my assumptions and it was almost as if I was waiting for a top down restructuring of medical education to make this situation better. What I now realize is that effective use of technology is not up to the faculty. Training can be facilitated by the University, but at the end of the day it is up to me to analyze my teaching environment, students, learning goals and outcomes. I have a responsibility to my students as an educator and it is up to me to rethink my use of technology.
In module B, we started off by learning about Pedagogical content knowledge (PCK) and Technological pedagogical content knowledge (TPCK). TPCK “emphasizes the connections, interactions, affordances and constraints between and among content, pedagogy, and technology” (Mishra & Koehler, p. 1025). This framework clearly defined my knowledge gap as an educator in the 21st century. Though it is always a work in progress, I was pretty confident with my PCK. What needed work was my Technological content knowledge (TCK) and Technological pedagogical knowledge (TPK). This allowed me to focus the remainder of my time in this course to begin filling my TPCK knowledge gap.
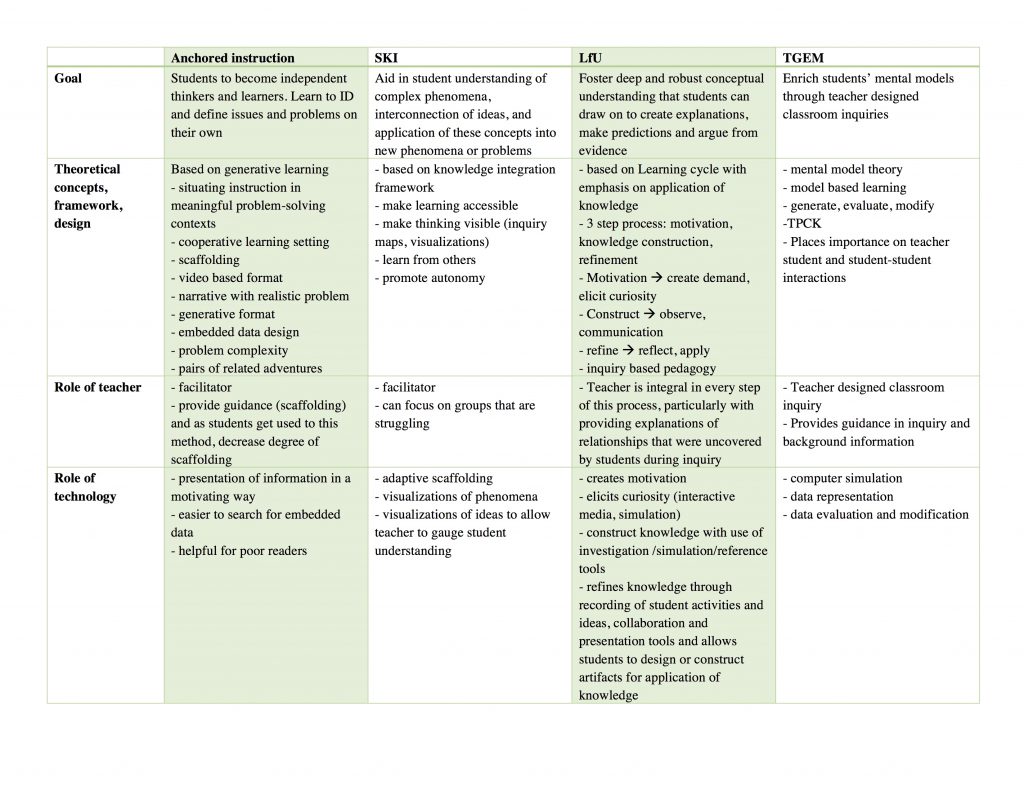
As I worked through Module B, I became familiar with different types of technology enhanced learning experiences (TELEs) that were used in STEM classrooms, as well as their underlying frameworks. All four were routed in constructivism, and all of them emphasized the importance of collaboration. In terms of technology, all methods used it as a way to present information to students, and each one allowed the students to interact with it in meaningful ways. Each TELE differed in the way and degree to which scaffolding was provided. On reflection, I think each one of these TELEs could have a place in medical education. The choice is TELE is dependent on the student’s level of knowledge, learning goals, cognitive and social affordances of each. I would also need to explore and test the use of these TELE in specific medical contexts. In my brief exploration of each, I believe I have increased my TPK though there is a long way to go. As Gary Ma pointed out in his Module B Synthesis post, “learning how to use these different tools to teach effectively is quite a monumental task”. But again, I must remind myself that the size of the task should not deter me from the task itself. For “[if] we teach today’s students as we were taught yesterday, we rob them of tomorrow” (John Dewey)
As pointed out earlier, all methods emphasized the importance of collaboration. Collaboration enables students to engage in discussions with others, which in turn can facilitate reflection (Edelson, 2001). This reflection is a key component of learning and improving understanding (Linn, Clark, & Slotta, 2003). In pre-clerkship medical education, which is mainly done in the lecture theatre, the majority of student time is spent individually. I observe many students passively listening to lectures as they look at the PowerPoint material on their personal laptops. Some are even doing other things during lecture time, such as browsing through Facebook. The readings, activities and discussion during Module B has really inspired me to change this, at least in the lectures that I participate in. I am hopeful that with this new found knowledge and enthusiasm, I will be able to make such changes, even with the constraints of the physical space (lecture theatre) and the overwhelming number of students. These changes could be as simple as posing a question to generate discussion in the middle of the lesson and encouraging the students to talk to their neighbour student. I think the trick to these questions would be to make them challenging enough to generate discussion but not too challenging that the students disengage as was pointed out by Linn, Clark and Slotta (2003) in their design of WISE.
Another theme that was emphasized in the TELEs was the role of the teacher as a facilitator. This is in direct contrast to many medical school lectures where the teacher is the disseminator of knowledge. Khan (2010), in her research on T-GEM found that the teacher viewed their role as a guide in inquiry. Similarly, CGTV (1990) saw the role of the teacher as a mediator of discussions and a guide to discovery. This again highlights the change that is needed in medical education. In order to “foster deep and robust conceptual understanding that students can draw on to create explanations, make predictions and argue from evidence” (Edelson, 2001, p. 355), they cannot be passive listeners in lectures. They need to engage in inquiry and experience the process of questioning, evidence-gathering, and analysis that echoes the scientific method. I was really inspired by the modelling of the scientific method in many articles that we read and would like to strive to achieve that in my classrooms. In order to achieve this type of active learning, I need to restructure the lessons I teach and change my role as a teacher to that of a facilitator, who guides students in their learning and assist in generating meaningful discussion and collaboration.
Making the concepts accessible was another theme that drew my attention. This was emphasized in all the TELEs that we studied. Knowledge can be viewed as tools, and “when people learn about a tool they learn what it is and when and how to use it. When people learn new information in the context of meaningful activities, they are more likely to perceive the new information as a tool rather than as an arbitrary set of procedures or facts” (CGTV, 1990, p. 3). Looking back at the many lectures in medical school that I observed, students were given decontextualized facts that they were then expected to draw upon when they encountered patients in the following years. We were providing students with inert knowledge, which is knowledge that can be recalled when explicitly asked to do so but is not used spontaneously in problem solving even though it is relevant (The Cognition And Technology Group At Vanderbilt, 1990). Though medical education has tried to compensate for this by adding problem based learning to their curriculum, the vast majority of “knowledge” is obtained in the inert, passive form through a lecture format. It is not enough for our doctors to be able to recall the pathognomonic physical signs of systemic lupus erythematosus. We need them to be able to see a patient, use their knowledge to ask all the pertinent questions, examine them, order the appropriate investigations, and manage them accordingly, all the while remembering that each patient is an individual and their values and beliefs need to be considered during the entire process. We are doing the doctors of tomorrow a disservice by continuing to teach them the way we were taught. We need to situate their learning in applicable contexts that are accessible in order to achieve a deeper level of understanding that goes beyond inert knowledge.
In Module C, we explored emerging genres of teaching, learning and digital technologies. Some of these genres are older ideas that are being elevated by advancements in digital technologies, such as augmented reality, virtual reality, and mobile devices. What stood out to me during this module was the sheer volume of these education technologies that I was unaware of. As I explored each one, it led me to look for similar technologies used in medical education. Though the volume is much smaller than that found for K-12 education and the vast majority is not free, it is growing. I am excited to explore more of these technologies, analyze their cognitive and social affordances for learning medicine, and integrate some of them into an active learning environment.
Embodiment, which is the physical dimension of cognition, and embeddedness, which is the interdependence of cognition and the environment, were new terms that I had not encountered until Module C (Winn, 2003). Winn (2003) goes on to explain that our sensory experience of the world is limited by our physiology. For example, we cannot see beyond certain wavelengths or hear sounds below or above certain frequencies. This is where artificial environments that create metaphorical representations can be useful to bring students concepts and principles that “normally lie outside the reach of direct experience” (p. 8). I believe this is particularly applicable when learning medicine. We examine patients and observe their signs and symptoms within our physiological constraints, but we must understand their condition, investigations, and treatments at microscopic and molecular levels. With information visualization, simulation and modeling technologies, these metaphorical representations are not only achievable but can be created to be dynamic and interactive. When metaphorical representations are depicted in a text book, they are two dimensional and static. In the context of diffusion and osmosis, it was found that students often fail to grasp many concepts such as the dynamic nature of this process (Friedrichsen & Pallant, 2007). However, when using a program such as Molecular Workbench, students showed a significant increase in their understanding of a variety of concepts and were able to easily transfer their new understandings to novel situations. I believe a similar level of understanding could be achieved by medical students if given the opportunity to interact with such representations.
I started this course as a disgruntled frustrated medical educator, but I feel as though I have completed my journey with a sense of hope. Reflecting back on this course, I have come to the realization that the only true barrier to effective use of education technology in the classroom was me. I used class size, lack of time, and lack of faculty driven guidance and assistance as excuses for my TPCK gap. Through this course, I feel that my eyes have been opened to the potential of various education technologies and TELEs. That being said, I also recognize that these technologies are tools and certain tools are applicable in certain situations and their usefulness can vary based on the user. As an educator, my role is to explore these technologies, analyze their affordances and use them in situations where it will benefit my students’ construction of knowledge. In addition, I need to see myself as a facilitator, and allow my students the freedom to explore, inquire, and challenge themselves while working together to problem solve and construct knowledge. I know that this will not be an overnight project, but I hope to continually make small changes and gradually achieve the type of active TELE that has been exemplified in this course.
References
Edelson, D. C. (2001). Learning‐for‐use: A framework for the design of technology‐supported inquiry activities. Journal of Research in Science Teaching, 38(3), 355–385. http://doi.org/10.1002/1098-2736(200103)38:3<355::AID-TEA1010>3.0.CO;2-M
Friedrichsen, P. M., & Pallant, A. (2007). French fries, dialysis tubing & computer models: teaching diffusion & osmosis through inquiry & modeling. The American Biology Teacher. http://doi.org/10.1662/0002-7685(2007)69[22:FFDTCM]2.0.CO;2
Khan, S. (2010). New Pedagogies on Teaching Science with Computer Simulations. J Sci Educ Technol, 20(3), 215–232. http://doi.org/10.1007/s10956-010-9247-2
Linn, M. C., Clark, D., & Slotta, J. D. (2003). WISE design for knowledge integration. Science Education, 87(4), 517–538. http://doi.org/10.1002/sce.10086
Mishra, P., & Koehler, M. J. (2006). Technological pedagogical content knowledge: A framework for teacher knowledge. Teachers College Record, 108(6), 1017–1054.
The Cognition And Technology Group At Vanderbilt. (1990). Anchored Instruction and Its Relationship to Situated Cognition. Educational Researcher, 19(6), 2–10. http://doi.org/10.3102/0013189X019006002
Winn, W. (2003). Learning in artificial environments: Embodiment, embeddedness and dynamic adaptation. Technology.