According to Edelson (2001), LfU is based on 4 theories of learning, which are:
1) learning takes place through construction and modification of knowledge structures
2) knowledge construction is a goal-directed process, guided by a combination of conscious and unconscious understanding of goals
3) circumstances in which knowledge is constructed and subsequently used determine its accessibility for future use
4) knowledge must be constructed in a form that supports use before it is applied.
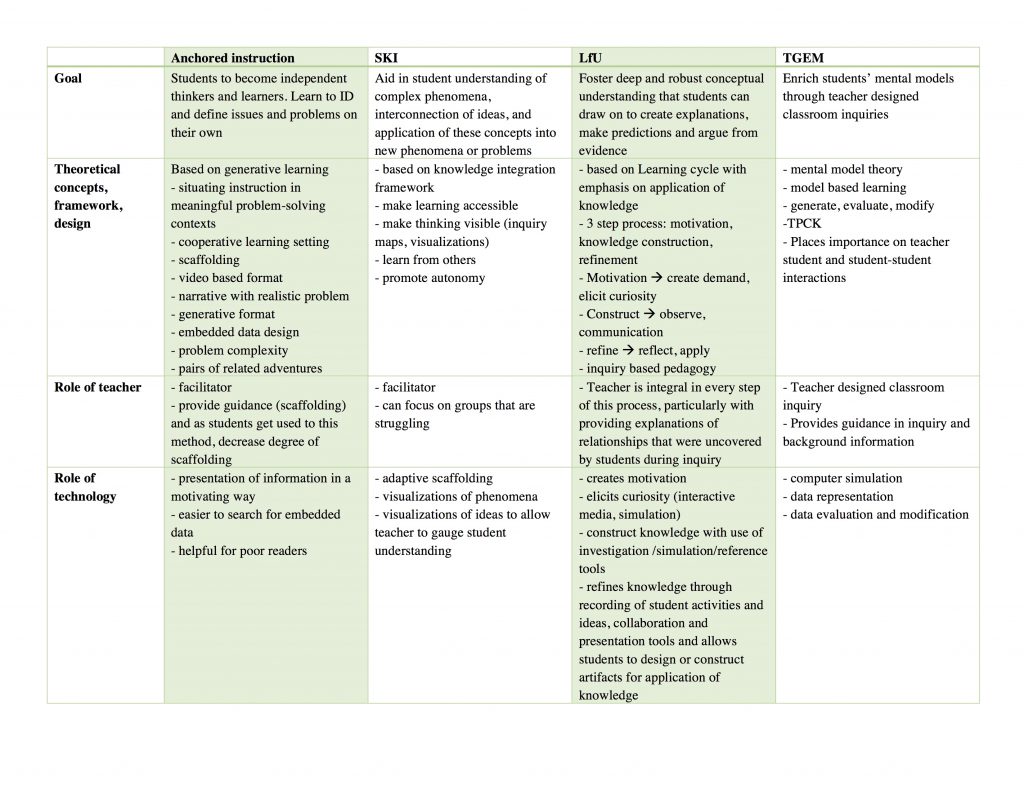
These principles underlie the LfU model, which is a three-step process involving
1) motivation
2) knowledge construction
3) knowledge refinement
In terms of technology, it plays many important roles within the LfU model. For example, it can play a role in eliciting curiosity (motivation), help students interactive with phenomena not possible in the real world which aids with knowledge construction and refinement.
So how would I apply it to a topic that I teach? The one thing that comes to mind is pelvic anatomy. Students tend to struggle with pelvic anatomy because it is quite complex and has multiple layers to it. I would start off by presenting students with a case of a patient who underwent surgery and shortly thereafter developed leg weakness and pain (this is actually one of the patient that presented to me early in my career). I would then have the students come up with theories based on their current knowledge level, regarding the cause of this pain/leg weakness. This is to draw their attention to their current level of knowledge and to have them recognize their limitations and thus increase motivation to learn. This would also create a context in their memory for integrating new knowledge (Edelson, 2001). Then I would use AnatomyTV, which is an interactive 3D anatomy resource (available through UBC at http://resources.library.ubc.ca/page.php?id=888) as my software of choice. This interactive resource that allows students to manipulate the body in 3D (select 3D Atlas —> Pelvis, then click female pelvis and perineum ~ tumble under 3D views from menu on the left to try it out!), which is really helpful, as most textbooks only present the learner with the upright position of the human body. This is not practical because in most gynecologic clinical practices, we examine patients and operate on them in the supine position, and thus knowledge of anatomy in this position is much more applicable. This program also allows the user to strip away all layers of the body and add them one by one, which allows students to understand how each layer relates to the other. I would also have student work in small group to promote interaction and discussion as this also aids in knowledge construction and refinement. Finally, I would have the students reflect on their initial theories, make any changes they feel are needed and present it as a group to the class and further apply their new knowledge to come up with a management plan for the patient. In this way, I believe I have applied the LfU principles to this topic.
References
1. Edelson DC. Learning‐for‐use: A framework for the design of technology‐supported inquiry activities. Journal of Research in Science Teaching. 2001;38(3):355-385. doi:10.1002/1098-2736