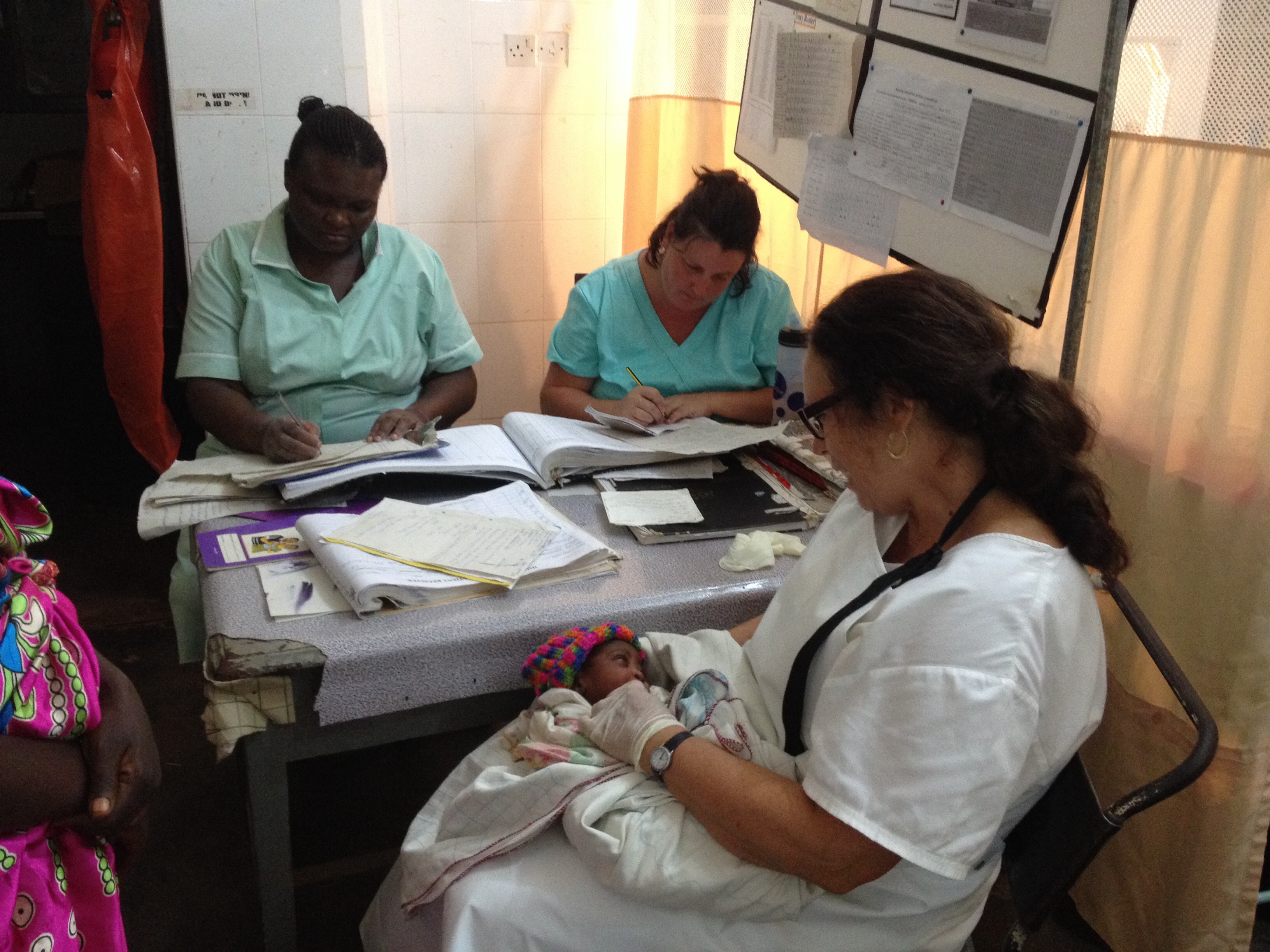
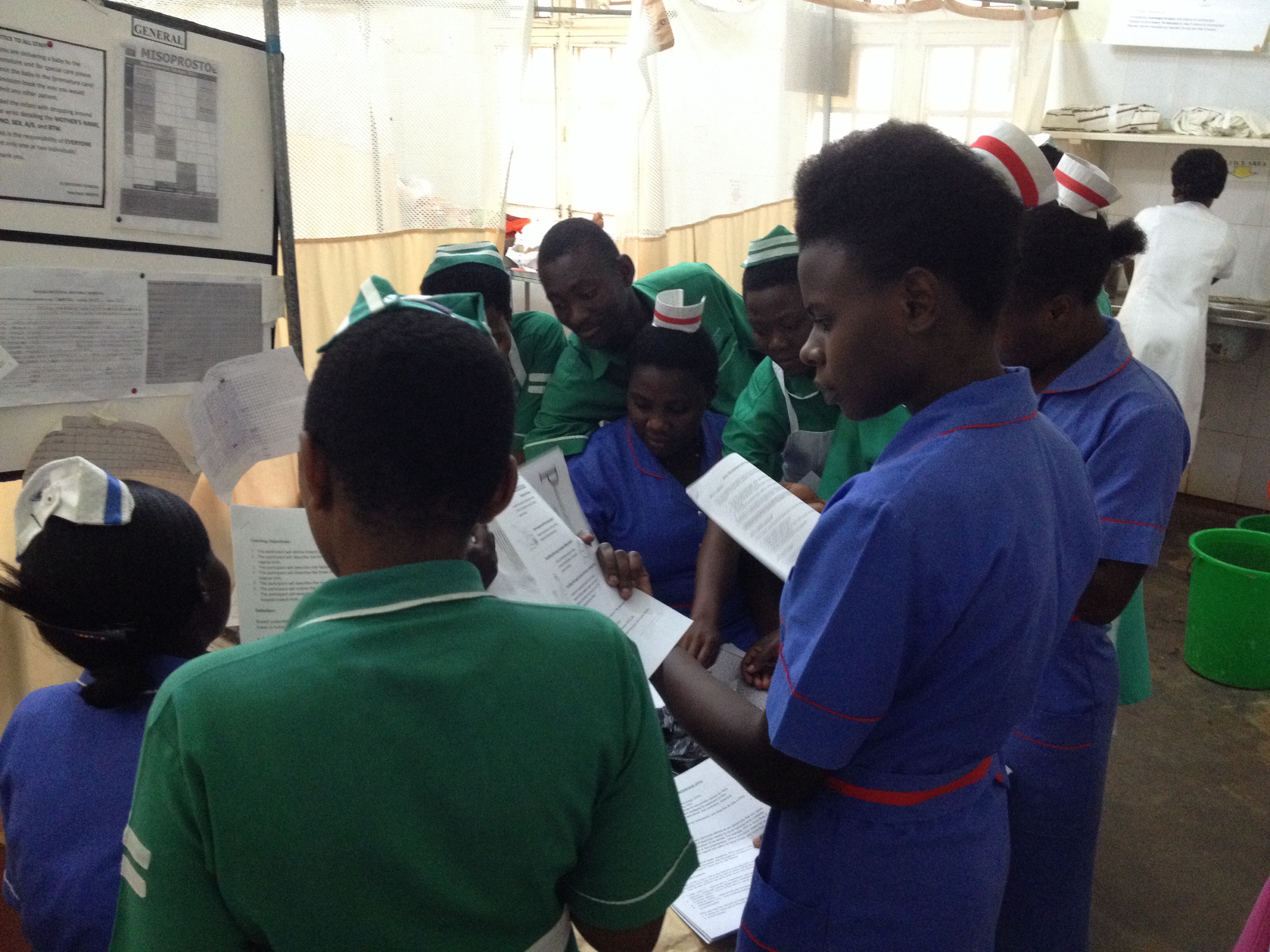
(note: pictures posted with the mothers’ permission)







(note: pictures posted with the mothers’ permission)
It is hard to believe the end is so near. Like many a great adventure it feels as though I have been here a lifetime and that I only arrived a moment ago.
I have gained so much experience and had so many experiences that I doubt I can describe them to anyone and yet they will profoundly inform the Midwife I am to become.
Today started out with a 30 minute resuscitation. It’s not my favourite way to start the day, but Lesley and I were working so well together and we had good bilateral air entry right from the start with a steady (if a little high) heart rate throughout.
Thank you thank you to all who donated toward resus equipment! It truly saves lives!
After 30 minutes the baby boy started breathing on his own and the Pediatrician assessed him and gave him a dose of antibiotics. He was stable for the time being, but we are going to check in on him over the next few days.
The rest of the day was filled with more births! (Imagine that!) we had a precipitous multip birth (one push and the baby came right out!), a slooooooowwww primigravida birth, another slllloooooooowwww primigravida birth, a speedy speedy multip birth in the admission room and an unexpected breech in the first stage room (Lesley and Beatrice worked wonders with that birth in not so ideal circumstances.)
I am continuing to learn a tonne, and my gratitude grows everyday to these mothers and to my midwife teachers.
Birth is wild. Women are strong. Babies are resilient.
Cathy – our fabulous instructor – posted a comment to our most recent gallery post. I tend to be a bit ‘wordy’ with my posts, and thought Cathy’s succinct summary of the past weeks was deserving of it’s own post!
—
“I have two more clinical days to work with Rachelle and Lesley at Masaka Regional Referral Hospital. We have dealt with every emergency in our Midwives Emergency Skills Course, as well as the “Advances in Labour and Skills Management’ (ALARM) course. This includes breech, twins, excessive bleeding before and after birth, hypertension, pre-eclampsia and premature deliveries. We have also attended older moms, 15 year olds, and worked alongside many Ugandan students who did not have preceptors with them and whose skills were at beginning levels. Shortage of supplies and human resources are the norm and there is always too much work to do. Our students are loving and caring to the mothers and will be strong midwives for women and families in British Columbia.”
Cathy Ellis, RM and UBC instructor
Today was my second day back in the delivery room after twelve days! We spent a weekend in Jinja (where I focused on white water rafting on the Nile!) followed by a week in Kampala (where I focused on antenatal assessments, observing fistula surgeries, and teaching workshops) followed by a weekend at Lake Mburu (where I focused on taking photos of zebras, leopards, and hippos!), followed by a virus that kept me in bed for a day. My first day back (yesterday) was quite interesting – my first ever 5x nuchal cord (cord was wrapped around the baby’s neck five times!) as well as my first experience of cord prolapse (Having to hold the baby’s head up off the cord while we rushed the mother to the OR was crazy hard to do! We had a positive outcome, though, and there was much cheering in the OR!) It’s been great to get back into the swing of birth.
Today:
1st STAGE ROOM BIRTH! The birth in the first stage room was totally unexpected. I went in to do a simple “early assessment” of a 15 year old primigravida (first pregnancy): palpation, fetal heart rate, maternal vitals, contraction pattern, and vaginal exam. After palpating mom’s belly it seemed her bladder needed emptying. She was unable to pee, so before I proceeded with anything else I catheterized her. As I did so I noticed her pushing… and… the baby’s head suddenly appeared!
“Whoop – there it is!” (lol!)
I was totally unprepared for birth, but Lesley was on it! I was already “sterile” from having just catheterized her so Lesley (who had been assessing a woman with severe hypertension also in the first stage room) speedily gathered the supplies we needed for birth: 10 iu oxytocin in a syringe, cord ties & a razor blade, baby blankets. The mom was 15 years old and her body was noticeably smaller than other women I’ve delivered. Her perineum was only about two centimeters long (short!) and I have to admit I was a bit nervous.
The second stage proceeded quite slowly (the stage where a woman is fully dilated and pushes her baby out), but when the baby girl was finally born she came with double nuchal hands – both her hands were in fists around her face! No wonder her head was slow to emerge! She came out pink and crying, and the placenta came (complete) a few minutes later. She did have a small first degree tear to repair, but overall it was a lovely birth!
TWINS! The twins were, as with the first birth of the day, unexpected (to me). I had just finished telling Cathy that I was starting to feel unwell and thought I should probably head home. I had stayed home sick the day before and suddenly felt the sickness returning. Cathy thought that was probably a good idea, but asked that before I left if I would insert an IV on the mom who had just arrived – a G3P2 pregnant with twins. We had just assessed her as 6 cm dilated and we wanted to get the IV in before we left. Women pregnant with twins are at increased risk for PPH (post partum hemorrhage) due to the distension of their uterus from carrying two babies, and being prepared with an IV can facilitate giving medication quickly should bleeding occur postpartum. Cathy asked me to do it because we have a little skills game we like to play called “3 for 3”. I had successfully inserted two IVs that day, and this would be my “3 for 3!”
I happily agreed.
A few minutes later, after having successfully setting up my “3 for 3” IV, the mom looked at me and simply said, “Omwana” (ie. baby). I lifted up the mom’s dress and again…
“Whoop – there it is!”
A baby was coming! She had dilated from 6 to 10 in about 15 minutes! My call for help came out like this: “Baby, coming out, now!”
Thankfully Cathy and Lesley were both free to come to my aid. In less than 10 seconds Cathy brought me sterile gloves to put on top of my nonsteriles and drew up two doses of oxytocin, and Lesley went to track down the woman’s baby blankets. (The hospital here does not supply blankets to receive babies; the women must bring their own. In this case this woman had neglected to bring her supplies with her into the delivery room, and it can take a while to track down her attendants out in the hallways/front lawn to get her supplies!) The baby was born very quickly so I grabbed the mom’s personal shawl to warm and dry the baby. “Twin A” was screaming just as we like, and though Lesley returned without having found the woman’s attendant and supplies she was able to retrieve one of our donor blankets from the storage closet to wrap the baby in, which was awesome. (Thank you donors!!!)
The thing about a woman birthing twins is that Twin A needs to have their cord cut and clamped right away. With single babies we prefer to do delayed cord clamping. This ensures the baby receives maximum blood post birth and reduces rates of anemia at the 6 month mark. With twins, though, you have to be careful. We did not know if the babies shared a placenta and amniotic sac. If they did, something called “twin to twin transfusion” can occur, and if the first twin continues to take in blood from the placenta after it is born there is a possibility that the second twin can lose too much blood. Because we were not prepared for the birth we didn’t have our clamps handy… but… I had clamps in my pocket for just such an emergency! Thankfully! I pinched the cord and Cathy went digging in my pockets and found two clamps. Perfect. We clamped the cord, cut it, and Lesley went off with baby to the warmer while we prepared for Twin B.
The next step with twins is to determine the position of the second twin. We palpated and could tell the baby was in a longitudinal position, which was good. If there’s one thing you don’t want it’s a baby in transverse lie. According to our palpation the baby was breech, and as I did a vaginal exam to confirm our suspicion I felt a foot. Alarmed I looked to Cathy and said, “It’s a foot! What are we going to do?” (I have it lodged in my mind that a baby in frank or complete breech are fine for vaginal delivery, but footling can be a problem.)
Cathy, in her calm and witty way, looked at me, smiled, and simply said, “It’ll come out!”
Sure enough not 5 minutes later Twin B’s two feet slid out of mom’s vagina – IN THE CAUL! I have never seen that! Breech-in-the-caul! Amazing.
We opened up the sac and proceeded to have a vaginal breech delivery. I remained hands off until I could see the scapula. Then I reached in and scooped out the anterior arm, rotated the baby slightly in the opposite direction by placing my fingers on the iliac crest and my thumbs on the sacral bone and rotating, and then scooped out the other arm in the same way. Then I got into the mariceau-smellie-veit-position with the baby resting on my left forearm with my two fingers on the baby’s mallor bones just inside the introitus and my right hand provided flexion on the occiput. This was only my second breech delivery, and I found this move much harder this time around! We had to ease the baby’s head out by rocking it quite a few times – something I don’t remember being taught in our training and I was so glad to have Cathy’s extensive experience at my side. Baby was born, and though a little slow to breathe at first, he came around within a minute and no resus was necessary.
With the birth of Twin B came a gush of blood and the placenta was right there – there had been a placental abruption! (And boy were we glad we had the IV already inserted!) We gave the mom 10 iu oxytocin IM as well as 10 iu oxytocin IV in 500ml Ringers lactate. We removed the placenta (monochorionic/diamniotic for those of you interested!), rubbed her fundus, removed clots and catheterized her bladder with an in-and-out. The fundus firmed up nicely so we quickly assessed for tears and found a small first degree tear that needed suturing.
All in all, another amazing birth and the mom was delighted with her boys.
During the excitement I had been able to put my feelings of sickness aside… but shortly after the delivery of the placenta and initial postpartum management I started to feel unwell again, so Cathy encouraged me to head out and she would finish up. I was grateful to be part of such a supportive team!
When Cathy and Lesley returned to our accommodations a few hours later they told me that the mom had started to bleed again after I left. They expelled numerous more clots and had to give another 10 iu oxy IV as well as 600 mcg misoprostil. Although we had used an in-and-out catheter, it wasn’t until they actually inserted a Foley (a catheter that remains inserted to continually drain the bladder) that the uterus fully firmed up and the bleeding stopped. Foley’s are in limited supply here in Masaka so we had been hesitant to use one at first… but lesson learned. In the face of bleeding when risk factors are present, get the Foley in if you have it…
What a day!
because you never know when you’ll need them…
(And the second most important item? – A fully charged phone!)


not really but it made for some good jokes
Last weekend we took a break and met up with our colleagues in Jinga at the Kingfisher resort. Friday was a long travel day and we concluded with a “joyfull reunion”, a swim (in front of an audience of 50 or so muslim school children) and dinner. It was also Angela’s birthday so we had another reason for celebration.
Saturday morning Alix, Zahra, Rachelle and I were picked up at 7:30 and transported to a spot further down the Nile. The Kingfisher resort is at the mouth of the Nile on Lake Victoria. We joined a group to go rafting down the Nile! We had an amazing day. It began with lessons on how to survive the overturning of our raft and Rachelle got a suprise ducking by our guide. Once he was sure we all knew what to do we started off. Immediately we reached the first rapid and our guide told us that unfortunately the river was too high and we were going to have to get out and walk around. We steered to shore and a guide grabbed our raft – but he couldn’t hold it and we shot backwards down the rapids! We were all shocked and exhilarated when we spat safely out the other end. Our journey continued with a leisurely drift and swim and a series of rapids. In one we flipped over entirely and in another we tipped to almost a 90 degree angle and everyone on the right hand side of the boat was lost, this included rachelle. The rest of us stayed in the boat, barely.
We ended with lunch about 2pm in a lovely spot over looking the nile and then were transported back to the kingfisher for more swimming, resting and visiting.
Sunday we took a lovely and sedate cruise out onto Lake Victoria, to the mouth of the Nile and up into the Nile. We saw many different birds, and some monkeys and enjoyed the beautiful scenery before returning to the Kingfisher for more swimming and lounging.
Later that same afternoon we departed for Kampala and the next stage of our journey.
We have now spent two weeks in Masaka Regional Referral Hospital. Some shifts have been light, but many have been tough – for a myriad of reasons.
In the midst of the challenge there are spurts of joy.
Tonight I am tired, and to be honest, I don’t feel like going in to the hospital tomorrow. Witnessing first hand maternal-infant health in Uganda has been eye-opening, challenging, and an incredible opportunity to solidify my knowledge and skill. But it’s hard work. Standing on the threshold of the delivery room you just don’t know what awaits you inside.
I have learned to look closely at the codes for my clients to know if they are HIV+ or not; many are positive. Today a 17 year old HIV+ mom gently asked us to make sure her baby would get treatment, and another 20 year old asked us not to let her attendant know her positive status.
When you are not used to them, these realities take a toll. I have only been here for two weeks. Two weeks. The midwives here face these stories – these women – day after day after day. And they are tired too. They are paid for 8 hour shifts, but are required to stay for 12 hours.
This weekend is our retreat weekend with the Mbale team. We’ll meet up in Jinja and have some fun together – and I am ready for a break! We will also have a clinical “case study” academic exercise and go through our midterm evaluations. Next week we’ll be in Kampala at Mulago National Referral Hospital facilitating teaching workshops and participating on various antenatal and delivery wards. I look forward to a change of pace. After that we’re back to our respective sites in Masaka and Mbale for until we head home early July.
Time is passing so quickly and so slowly at the same time. It’s sometimes overwhelming and sometimes super gratifying. But for right now, I’m so happy to be going to bed.
With the head midwife
Head midwife pops in to see how things are going in the labour & delivery ward. Cathy and Rachelle are attending a woman in 2nd stage to deliver her baby. No other midwives are present in the ward.
Cathy: “We should let you know that we will be leaving after this birth, but the two women in Beds 2 & 3 are about to have their babies.”
Head midwife [as she walks out of labour & delivery]: “We shall pray for them.”
Between head-midwife and student midwife
Student midwife: “There is no stretcher to take this woman to theatre.”
Senior midwife: “Midwife – walk your woman.”
With a labouring woman
Winnie: “Sista – help me!”
Rachelle: “I’m here.”
W: “Help me.”
R: [puts counter pressure on laboring woman’s back.] “I am here. You are doing great.”
W: “I’m dying!”
R: “You’re not dying. You are having a baby!”
W: “When?”
R: “Today! You will have your baby today.”
W: “What time?”
R: “I don’t know what time!”
W: “Tell me when my baby will come!”
R: “I don’t know what time, but it will be today.”
W: “I’m dying!”
R: “No, you are not dying. Here is some sugar-tea. Do you think you can lie on your side?…”
W: “Don’t leave me!”
R: “I won’t leave you.”
[Baby is born about 45 minutes later.]
W: “I am so happy. Thank you. I am so happy.” [Big smiles.]
R: “I am so happy too!
With a stranger at the bank
After a friendly exchange with a Ugandan woman at the bank…
Friendly stranger: A man once said to me, “You are strong like a man.” But I said, “You are mistaken. I am woman.”