
Day 4 – Child Undernutrition
Presented by Ann-Sophie Iuel-Brockdorff who is currently working in the nutrition department of the Exercise and Sports faculty at the University of Copenhagen (I got her email.. yaay!)
UNICEF Definition:
Undernutrition is defined as the outcome of insufficient food intake (hunger) and repeated infectious diseases. Undernutrition includes being underweight for one’s age, too short for one’s age (stunted), dangerously thin (wasted), and deficient in vitamins and minerals (micronutrient malnutrition).
Before the lecture, in our binders we were given a few readings that we were supposed to (ahem.. supposed too…) read the night before the lecture. The readings included
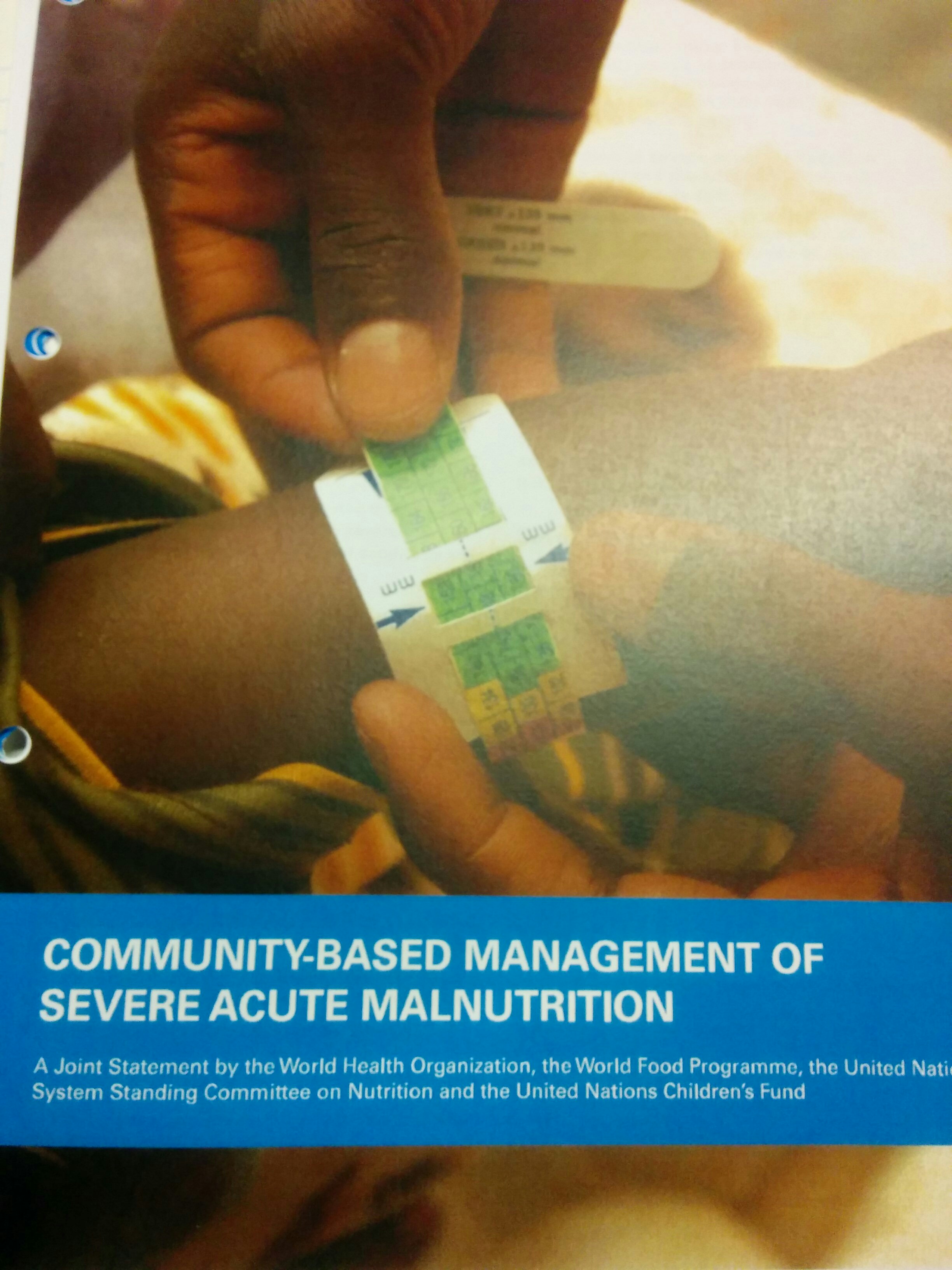
- Community-based management of severe aute malnutrition – a joing statement by the WHO, the World Food Programme, the UN system Standing Committee on Nutrition and the UN Children’s Fund, 2007
- WHO child growth standards and the identification of severe acute malnutrition in infants and children – a joint statement by the WHO and the UN Children’s Fund, 2009
- Infant and Young child feeding. Model Chapter for textbooks for medical students and allied health professionals. WHO 2009 (online)

Some nutrition related numbers to show the matter of urgency
- 800 million people are starving in the world today
- 195 million are children under 5 years of age – children are more vulnerable!
- Malnutrition is responsible for:
- 45% of all child deaths (3.1 million deaths)
- 11% of the total disease burden
- Good nutrition early in life is essential to children for
- Survival
- Attaining development potential
Remember those millennium development goals we went through last post? Well we also went through those again in this lecture and focused on some related ones to nutrition…
- In 2002 – 2015
- Eradicate extreme poverty and hunger
- Reduce child mortality
- Improve maternal health
- Combat HIV/AIDS, malaria and other diseases
- After 2015
- End poverty in all its forms everywhere
- End hunger, achieve food security and improved nutrition and promote sustainable agriculture
- Ensure healthy lives and promote well-being for all at all ages
But what are the reasons for malnutrition?
UNICEF has a framework for the causes and consequences of malnutrition which looks like this:
Basically the reasons for malnutrition include: Poverty, disease, natural disasters, war, gender inequalities, education, maternal care, orphaned at a young age, population displacement, lack of care/parent/role model, lack of food, poor food quality and over population in small areas. Looking at the figure above you can see how the framework is put together and what the layout is. The main point is that all these reasons lead to the same thing – malnutrition (especially in children) and increased prevalence of disease and increased mortality (especially in children). All these points are extremely important, quality and quantity of resources, whether it be humans, workers, economic, organizational, etc, all play a big role in access to food, quality of food, education on health and nutrition, and so on.
In case you haven’t taken any nutrition courses or aren’t sure how starvation works, here is a brief run down:
- Carb storages deplete within hours, usually around 6 hours after eating our bodies digest food and break down glycogen (making energy) – key organs then get energy from fat and muscle (the brain is fed from glucose that comes from the muscles and glycerol, then from ketones made from the fat stored in the body (but this can be dangerous and lead to ketosis eventually). Fat is linked to survival during starvation – muscles are linked to survival during infection (due to increased protein breakdown – seen in urine samples).
- Glucose stores can last up to 24-48 hours (although most stores are depleted in 6 hours). Overall, prolonged starvation affects every organ. After 3 days of no food, your body will enter into starvation mode and your body will begin to enter ketosis, elevating levels of ketones in your body. Ketones are produced from fatty acids when liver glycogen is entirely depleted and used for energy. Your brain will use the last of the remaining glucose – the brain uses about 120 grams of glucose every day.
- When glucose is low or depleted the brain will turn to energy from ketone bodies, getting about 30% of its energy from them. Past this your body turns to breaking down muscles for protein (wasting away the muscles) and conducts gluconeogenesis, making glucose from the protein building blocks (amino acids). By this time though, your metabolism has slowed down so much to the point that your body uses the smallest amount of energy possible. Basically you may be able to survive for up to 3 weeks or longer, depending on if you are hydrated or not. Of course you also have to take into consideration that in many places where malnutrition is prevalent, there is no clean water or sanitation to keep the population hydrated.
- There is also the point in which your immune system weakens due to the lack of vitamins and minerals (micronutrient malnutrition).
- At this point two acute diseases occur due to starvation (associated with wasting)
- Marasmus: a form of severe malnutrition and calorie/energy deficiency.
- Characterized by loss of muscle mass, almost no subcutaneous fat, prominent ribs and limb joints, irritability and edema
- Kwashiorkor (commonly seen): caused by not consuming enough protein
- Characterized by fatigue, oedema in the legs, arms and around the eyes (can represent up to 30% of body weight – changing accuracy of readings), pitted oedema, dermatosis of the skin and a decrease in muscle mass
- If there is Chronic Malnutrition it is associated with stunting
- Characterized by an okay weight/height ratio, but their height for their age is under – stunted growth
- Marasmus: a form of severe malnutrition and calorie/energy deficiency.
- At this point two acute diseases occur due to starvation (associated with wasting)
Most families in urban areas (example: a family of 4) live off of around $200-$500 per week, while a family of 6 in certain developing areas live off of approximately $1.44 per week (a chocolate bar a week for us)
Quantity vs. Quality
- Macro-nutrients (fat, carbohydrate, protein)
- Micronutrients (vitamins, minerals)
- There are over 40 nutrients that are essential to your health – if any of them are deficient in your diet then a person can and usually will be unhealthy and have a lowered resistance to disease, infection and bacteria, especially in developing countries.
How to test for malnutrition
- Anthropometric measurements
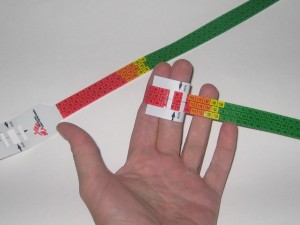
- Mid-upper arm circumference (MUAC)
- Fast and efficient
- Good predictor of risk of death: <115 mm
- Oh my gosh! We got to use the measuring tapes that they use and look at them.. think about 115 mm (pretty small) but when you see it in real life, that tape at 115 mm barely fit around 2 of my fingers and that represents a malnourished child’s arm. Could you imagine seeing someone with an arm that small
- Mid-upper arm circumference (MUAC)
- Weight for height (acute malnutrition – wasting)
- Indication of current health status
- Disadvantage: lower values for children with long legs – risk of overestimation of malnutrition in certain populations
- Modified by the presence of oedema
- Height for age (chronic malnutrition – stunting)
- Height compared to age group
- Reflects slowing of skeletal growth
- Indicator of poor social conditions or repeated exposure to chronic diseases, infections, poor feeding
- In adults
- BMI or MUAC
Assessing nutritional status in a population
- Evaluation of the nutritional status of children less than 5 years
- MUAC
- Will help to estimate the prevalence of Gobal Acute Malnutrition = MAM and SAM
- Necessary for determining and planning intervention strategies
- Evaluation of the food resources and coping mechanisms of the population
- Food security = access by all people at all times to sufficient, safe and nutritious foods for active and healthy life
- Looking at a calendar throughout the year for that city to know when crops are good, when rain is there, when and what diseases are prevalent.
- Nutritional survey coupled with a retrospective mortality survey
- Food program: general food distribution/blanket (targeted feeding distributions) feeding
- Insufficient food availability
- Objectives: to cover basic nutritional needs within a population
- To preserve and restore regular livelihood
- To prevent deterioration of nutritional status
- To preent morbidity and mortality due to malnutrition
- Food program: general food distribution/blanket (targeted feeding distributions) feeding
- General: – full ration (2100 kcal, good quantity and quality)
- Blanket: min 500 kcal/family member/day – target is children < 5
- Feeding programs: therapeutic feeding programs/supplementation feeding program
- General population – at risk – malnutrition are all affected by therapeutic feeding program/supplementation feeding program, blanket distributions and general food distributions.
Ready-to-Use Food revolution!
- Nutritious peanut paste ( F-100 + iron)
- Ready to eat with no preparation
- No content of water, decreased risk of contamination
- Individual packaging
- Increased coverage and capacity
- Actually tastes pretty good – but I, Rebecca Hayman, am a Peanut Butter-aholic. I could eat peanut butter all the time it is just the best thing ever, so of course I liked this little peanut paste pack!
After all of this we went through a few case studies and examples of in and out patients (who would be treated in the hospital or who would be treated with these nutritious peanut packs and be sent home with a certain amount of them.
When patients come in with malnutrition, how do you treat it?
- You have to be careful of refeeding syndrome
- Leads to heart failure
- Have to start slow – 2 phase program
- Phase 1 (low kcal milk powder [F-75} 8 times a day – no other food allowed)
- Transition to F-100 (6 times per day)
- Phase 2 (F-100 – 200 kcal/kg/day – want to see weight gain, can introduce other food products and prepare for outpatient treatments)
- Treat/prevent hypothermia
- Treat/prevent hypoglycaemia
- Treat/prevent dehydration
- Correct electrolyte imbalance
- ReSoMal
- Treat/prevent infection
- Correct micronutrient deficiencies
- Start cautious feeding
- Achieve catch up growth
- Provide sensory stimulation and emotional support
- Prepare for follow-up after recovery
- Have to start slow – 2 phase program
- Leads to heart failure
Conclusion
Malnutrition is a global health problem, and should be treated as a public health problem in many parts of the world
1/3 of all child deaths is due to malnutrition
Malnutrition can cause irreversible damage to the physical and mental development
Window of opportunity from conception to 2 years
Malnutrition is a clinical condition, demanding both nutritional and medical therapy
Malnutrition is a curable condition
It’s almost the weekend! Woo! All this talk about nutrition and I am in Denmark, making plans to go eat Danish food and buy some Danish pastries, with coffee of course. How sad is that.. but then again, I am pretty excited to try these pastries.


Went to a small bakery by my house here in Frederiksburg after class and bought a coffee and two pastries. Walked all the way home before I took a bite because I just had to take a photo for you! But I almost died on the way home… I guess there is a big cycling race? Or something? And I.. of course thinking of my pastries I could be enjoying, saw the green walk light so I start walking and all the sudden a bunch of motorbikes started coming and honking at me to get out of the road and seconds later hundreds maybe thousands of cyclists came racing by followed by their team cars carrying the spare wheels and bikes behind the group. This race went on all day with huge groups going one after another past my house (I took photos for you of course..)


Later we wandered, a few friends and myself, to the city. We saw the harbour, saw some pretty buildings including the palace and many beautiful statues and buildings. I walked through the outer part of the palace and took photos of the Queen’s house, the Prince and Princesses’ house as well and a few other beautiful buildings. We also went into the Queen’s garden and enjoyed the huge flower displays and beautiful stone work. After we walked over to Christiansborg tower and “climbed” up to the top – we took the elevator.. haha. It is one of the tallest church towers (standing at 106 m). We looked and found many things from up there, including Sweden! Now I can officially say I got to see Sweden (that counts right?). Here are a few photos of my ventures and friends!







Myself, Bridget (my Australian flat-mate) and Thomas (a German Doctor from Berlin)

Myself and Brendan (Doctor from Holland you met earlier) on top of the Christiansborg tower!

My other flat-mate from England, Camilo, enjoying the fact that you can drink everywhere here in Denmark (anywhere.. like on the street you can just carry about beer or wine or whatever you want! I love it – I don’t drink but it’s still awesome). Here we were at Stella Polaris – a electronic music festival enjoying some picnic foods and wine with some interesting music and meeting new friends!
