
This was probably one of my most favorite workshops that we did. This workshop was a cross between a lecture and multiple discussions within small groups then with bigger groups and then between the professor and the whole class. The topic… Triage.
Now I have not worked or been trained in anything like this, I know how to take heart rate and blood pressure and that’s about it… but I so rocked these discussions because apparently I am a ‘realist’ or.. a cold hearted evil lady – either way triage would suit me said Henrik Kahler (the lecturer).

- The main purpose of this lecture and workshop was to give us a simple tool, which you can use in an emergency situation with many casualties to save as many lives and limbs as possible.
Why is triage so complicated – because you have to initiate the correct triage and get the right treatment to the right people in the right amount of time! You really need to know which is more critical – who needs to be treated first and who can wait a little bit longer
- Trauma is the most common cause of death (between birth and the age of 40/50 years)
To start we will cover some of what the lecture portion was like then I will give you guys some of the discussion topics and examples we worked through and see what you all say!
What is triage?
- A process of prioritizing patient treatment during mass-casualty events / multiple casualty incident
- Multiple casualty incident
- Patient care resources are overflowing and being overextended but not overwhelmed – helpers still available and resources are still available if needed. Triage is here used to focus on identifying those who have the MOST life-threatening injuries
- Mass casualty event
- The patient care resources are overwhelmed and cannot be supplemented. Triage methods are focused on identifying casualties with the greatest chance to survive.
- Multiple casualty incident
Basic principles? – Think critically
- How serious is the casualties conditions?
- Is the condition life threatening?
- Is it limb threatening?
- How is salvage ability?
- Resources available?
- Time available?
- Never forget that the given information you have may not be complete. Try to use everyone around you including patients with minor injuries. MAKE A DECISION – any decision is better than no decision at all. Of course, don’t forget that triage is a dynamic process – things are always changing, always moving and there is always something happening!
Medical intelligence – things to think about and know
- Geographical issues
- Altitude
- Borders – problems or conflict with surrounding countries
- Transport infrastructure
- Airports
- Road conditions and availability
- Evacuation routes – where are they and are they safe
- Medical infrastructure – capacity and capability (resources)
- First aid stations
- Primary ward
- Medical transport
- Education of medical staff
- Hygiene problems
- Water availability and safety (sanitation)
- Disease pattern in the country
- Dangerous animals
Know the expected injury patterns according to the disaster at hand
For example:
- Drought Heat – exhaustion, stroke, dehydration, renal failure, malnutrition and starvation
Categorisation of patients – criteria
- The nature and life-threatening urgency of the patients’ present condition rather than the order in which they arrived, as is normal in emergency care facilities
- The potential for survival or the prognosis identifying those patients with the most urgent need for care, which is counter balanced by the availability of health care resources. This concept is critical and can greatly influence the overall survival rate of disaster victims.
- How to group casualties
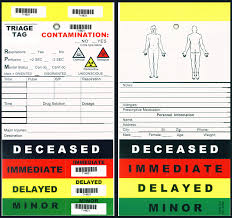
- T1 – Red marker: Patients whose condition is life threatening and should be treated immediately
- T2 – Yellow marker: Patients whose condition is serious and should be treated quickly
- T3 – Green marker: Patients who do not have a life threatening condition and can wait
- T4 – Black marker: Patients who have died
- T5 – Blue marker: Patients who are awaiting final clarification (between T1 and T4)
- You can also make your decisions based on the ABCDE method and some anatomical criteria – This method allows for rapid precise assessment of the patient, sort through need and capability, helps to set an arrangement of transfer to definitive treatment and ensures optimal treatment.
- A: Airway with c-spine protection (ensuring free airway)
- B: Breathing – normal breathing rate is approx. 12-16 breaths per minute with normal breathing sound bilateral
- C: Circulation – Normal BP, normal skin colour and normal organ perfusion
- D: Disability/Neurologic Status – Consciousness or paralyses
- Using the Glasgow Coma scale to get an idea (score) of consciousness
- E: Exposure or Environment – where are they, what were they and are they exposed to right now
- High vs Low energy Trauma – Things to look for and realize before categorizing the patient
- . Kinetic Energy – dependent on mass and velocity
- If you have low energy you’ll have a straight through wound – a bullet enters and it exits (if nothing is in the way of course)
- If you have high energy you’ll see an entrance wound then usually a bigger or more jagged and messed up exit with more damage on the inside
- Blunt vs penetrating trauma
- Blunt = no skin perforation (getting hit by a falling log in an earth quake)
- Penetrating = skin trauma (being stabbed or shot in war)
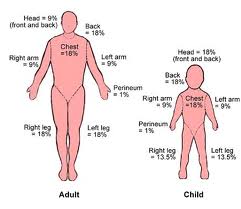
- Cold and Burns
- Follow the rule of nines
- The human body is split up into sections and given a percentage
- Another thing to consider: if you have a burn patient – Add up the percentage scores then add it to their age – if it sums up to 100 then the likelihood that then patient will survive is greatly decreased.
- Follow the rule of nines
Summary: (almost at the good stuff don’t worry!)
- Detailed examination of the patients is not always possible, but a decision must be made! Remember any decision is better than no decision
- Act according to the decision made
- Use the ABCDE method for prioritisation
- Triage is a dynamic process
SCENARIOS! Exciting!
- You are in a small village. The initial earthquake happened ½ hour ago. The local hospital has minor damages and can be used, but has only very limited resources. A better and larger hospital is 200 km away and can receive casualties.
- You are called to a triage area at a house, where 5 persons are injured in a gas explosion. You quickly survey the situation and determine that the patients conditions are as follows:
- Patient A: A young man is screaming “Please help me, my leg is killing me”
- Patient B: A young woman is cyanotic, tachypneic and breathing very noisily
- You are called to a triage area at a house, where 5 persons are injured in a gas explosion. You quickly survey the situation and determine that the patients conditions are as follows:
- Patient C: A 50 year old man is lying in a pool of blood with his left trouser leg soaked in blood
- Patient D: A young man is lying face down on the ground
- Patient E: A young man is swearing expletives and shouting that someone should help him or he will call his lawyer
- How will you prioritise treatment and evacuation? The first ambulance is available now and can take 2 casualties. The next two will arrive in 1 hour.
- So…. Which 2 do you choose to go right away, and which 3 do you treat while they wait?
- Remember all the stuff above and think it through
- Patient A – generally we don’t know.. maybe a broken leg – not so serious
- Patient B – has airway and breathing problems and is probably the most critical – serious! She is cyanotic, not getting enough air and there could be damage to her trachea or lungs
- Patient C – circulation problem, looking at the amount of blood and his leg, there could be a penetration to a major artery in his thigh, or an open compound fracture – could potentially be serious
- Patient D – we don’t know – no movement could mean he is unconscious or he is dead
- Patient E – tell him to shut it and help out is what I said and Henrik agreed. This guy can actually be very helpful if he will calm down, he could help patient A with the leg, or even if he is okay with it go check patient D to see if he has a pulse or not while you deal with the most serious patient (B).
- So who would you send?
- I said – Patient B and C – they are the most critical at this point. Check patient D and deal with him accordingly. Check patient A and deal with accordingly and really you can check patient E.. maybe for like.. Bruises and shock but I’m pretty sure he’s find and just annoying (and needs to shush).
Scenario 2:
- During the earthquake an explosion and fire has involve 2 cottages in a small village and 5 persons are badly involved. You are at the scene with limited resources but with possibility to transport to another town, where further initial treatment can be initiated. Two casualties can be evacuated immediately and the others after 1 hour. The injured patients are:
- Patient A: a 45 year old man is coughing. Hairs on his face and head are singed. His voice is clear. He can walk around. Some pain due to burns on hands and legs, which have erythema and early blister formation.
- Vital signs: BP 130/90 mmHg, HR 100 bpm, RR 25 breaths/min
- Patient B: A 8 year old crying boy with 20% surface area with 2nd degree burns mostly related to the legs, nothing in the face
- Vital signs: BP 110/70 mmHg, HR 100 bpm, RR 25 breaths/min
- Patient C: A 60 year old man is coughing, hoarse and expectorating carbonaceous material. He is unconscious and only reacts to painful stimuli. Burned area 40%, mostly second degree and mostly related to the chest and abdominal walls and both legs
- Vital signs: BP 80/45 mmHg, HR 130 bpm, RR 30 breaths/min
- Patient D: A 19 year old man is obtunded. He responds to pain when his right leg is moved. No other damages
- Vital signs: BP 140/90 mmHg, HR 110 bpm, RR 32 breaths/min
- Patient E: A 45 year old woman with pain related to pelvis. She is awake and reports pain in her pelvis. There is clinical evidence of fracture, and she also complains of abdominal distension and it hurts when palpated
- Vital signs: BP 130/90 mmHg, HR 90 bpm, RR 25 breaths/min
- Patient A: a 45 year old man is coughing. Hairs on his face and head are singed. His voice is clear. He can walk around. Some pain due to burns on hands and legs, which have erythema and early blister formation.
- Alright! GO! Who would you take first? You can chose only 2 for the first transport.
- My thoughts:
- Patient A: singed facial hair – potentially very serious because this means that most likely he has burns in his throat or lungs from breathing in which there was high heat near his face.
- Patient B: burns on the body – not super serious (I know I sound a little cold hearted but it is triage and he will probably survive either way)
- Patient C: 60 years old + 40% burns on his body = 100 – chance of survival greatly decreased. He is also unconscious and coughing up material – Very serious but a low chance of survival (again.. cold hearted but you can’t waist resources in these kinds of situations). Also his BP, HR and RR are all off – bad signs!
- Patient D: Head trauma? Shock maybe? BP is a little off, increased HR – maybe needs more assessment but nothing coming up right away as serious
- Patient E: Pelvic fracture with distension in the abdomen! SERIOUS! Most likely internal bleeding which can kill her very quickly and she needs to be treated right away.
- So who were my 2 choices? Well
- Patient A and patient E. Sorry to the old man and the screaming child but I can deal with the child and the unconscious guy after I send these two off and I can do my best to keep the older man alive or comfortable until the next ambulance arrives.
Triage is a hard thing, making those choices in real life would be 100 times harder but it is a job for someone who is realistic and a critical thinker. It is all about the situation and the decisions made, and sticking to those decisions!