
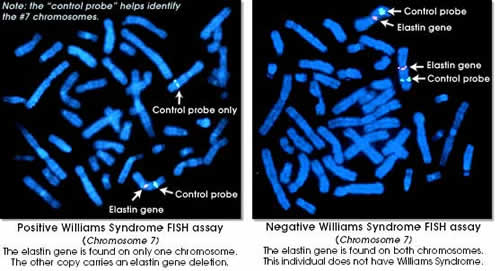
Williams Syndrome is a rare non-fatal congenital condition in which affected children are mildly to moderately retarded and score below average on IQ tests. They usually read and write poorly and struggle with simple arithmetic, yet they display unique abilities in other areas of intelligence, especially emotional intelligence involving socializing and empathy. The disorder affects males and female from all racial backgrounds at an equal probability.
The disorder is caused by deletion of a tiny piece from one of the two copies of chromosome 7 present in every cell of the body. Twenty-give or more genes are deleted and loss of one in particular (ELN) which codes for elastin, a connective protein gives rise to cardiovascular problems.
Such cardiovascular problems include heart murmurs and narrowing of major blood vessels, and supravalvular aortic stenosis, a constriction of the aorta. Babies may have difficulty feeding or suffer from stomach pains and hernias. As they develop, they show delayed physical and mental development with unsteady voices. They walk awkwardly for the rest of their lives and fine motor control is impaired. They are also highly sensitive to noise, grow to a shorter height than average and seem to have gray hair and wrinkles earlier. Lifespan for Williams patients is shorter than average due to the complications from these medical problems, but not from the Syndrome itself.

Williams patients usually have vocabularies larger than expected for their mental age and tend to be more expressive than normal children. However, they typically do poorly on tasks involving visual processing such as coloring and copying drawings. The brain anatomy of Williams syndrome patients is normal, but the total volume is slightly reduced. The areas that seem to be unaffected include the frontal lobes and a part of the cerebellum called the neocerebellum, as well as parts of the temporal lobes known as the limbic area, and the primary auditory area.
Study of this syndrome has shown that low IQ scores can indeed cover the existence of other skills and capacities. And it thus serves as an example that other so-called mentally disabled individuals could have lots of potential waiting to be discovered if only researchers and society take the time to look for and nuture them.
References:
Hemizygosity at the Elastin Locus in a Developmental Disorder: Williams Syndrome. A.K. Ewart et al. in Nature Genetics, Vol. 5, No. 1, pages 11-16; September 1993.
http://children.webmd.com/williams-syndrome-11011
{kind=link}