I’ve been meaning to post this but I completely forgot. While I was researching AR and it’s use for medical education, I came across this cool app. I haven’t tried it yet, but I think it has some potential. Anatomy of the heart and electrophysiology are tough subjects for medical students and I can’t wait to try this out to see if it would be helpful for my students!
Author Archives: momoe
T-GEM, NetLogo and public health
This week, I found myself really intrigued by NetLogo, especially the model on AIDS. I wanted to use this in a lesson on public health using the T-GEM approach (Khan, 2010).
Target audience: medical students
Topic: Public health
Lesson:
Step 1 – Introduction
Students will work in groups of 3-4 during this lesson. I would introduce the lesson by giving them the following scenario:
“ The CDC has just announced that a new retrovirus has emerged. No treatments for this virus has been established. It acts similarly to HIV in that it is sexually transmitted and the use of condoms significantly decreases the risk of infection. Infected individuals are initially asymptomatic, but later develop an immune deficiency, just like AIDS. A test has been developed to detect this virus but infected individuals only test positive 3 months after infection. You are public health officials who have been tasked to identify the most effect method to keep infection rates as low as possible.”
Step 2 – Prediction/Generate
Based on their current level of knowledge, students will be asked to predict methods that will be effective in minimizing the infection rate. They will likely come up with a few ideas, but will be asked to narrow it down to just one (given our current budget issues), based on their group discussion. This will then be presented to the rest of the class
Step 3 – Evaluate
Students will then be asked to use the NetLogo AIDS model to run their prediction. They will then explore other variables (condom use, frequency of screening, etc) to see if changes to these variables cause the desired effect (decreased infection rate). Based on the data, students will start to understand the relationship between these variables and infection rate.
Step 4 – Modify/Reflection
Students will then be asked to go back and look at their original predictions, and modify it as they see fit. Students will reflect on their initial predictions and their modified predictions to address any misconceptions they had at the beginning of class.
Step 5 – Peer review
Groups will then present their finial recommendation as public health officials and receive feedback from the remainder of the class.
References
Khan, S. (2010). New Pedagogies on Teaching Science with Computer Simulations. J Sci Educ Technol, 20(3), 215–232. http://doi.org/10.1007/s10956-010-9247-2
An argument against Globe as anchored instruction
I would like to disagree with the statement that Globe is an example of anchored instruction. If you look at the definition of anchored instruction superficially, one would have to agree that Globe qualifies. However, I believe that on a deeper level Globe does not embody all of the qualities of anchored instruction that the Cognition and Technology Group at Vanderbilt (CGTV) had in mind when they created the Jasper series.
Anchored instruction is where “instruction is situated in engaging, problem-rich environments that allow sustained exploration by students and teachers” (CGTV, 1992, p. 65). Based on this description, Globe certainly seems to meet the requirements. It provides a very engaging, problem-rich environment, and due to its many facets (atmosphere, biosphere, hydrosphere, pedosphere), sustained exploration can be attained. In addition, Globe provides an environment that allows communication between experts, students and teachers from diverse backgrounds, and this helps to build collective understanding. This is another important feature of anchored instruction.
Where Globe seems to diverge from anchored instruction is apparent when looking at the goals that CGTV had in mind when creating the Jasper series. CGTV’s aim was to help students learn to become independent thinkers and learners. They wanted students to learn to identify and define issues and problems on their own, in a generative fashion (CGTV, 1992). I would argue that students who participate in Globe, do not achieve this goal. The main activities in Globe centre around collection of data by students using a prescribed protocol that has been established by Globe researchers. This prescribed protocol is necessary to ensure that data collected by students is reliable and can be used by Globe researchers. I also took a look at some learning activities that students can perform. These documents provide teachers with a guide on how to introduce certain topics, gives step by step instructions on how to conduct the lesson, and possible ways to assess students on these activities. There seems to be a great deal of scaffolding in comparison to the Jasper series, which may hinder the notion of generative learning.
Overall, I believe that Globe is a very engaging community and does bring environmental science research close to home for students. I think that it is a very innovative endeavour and certainly has a place in STEM education. However, I cannot agree that it falls within the realm of anchored instruction.
References
Cognition and Technology Group at Vanderbilt (1992a). The Jasper experiment: An exploration of issues in learning and instructional design. Educational Technology, Research and Development, 40(1), 65-80
The importance of gestural congruency in embodied learning
For lesson 1, I decided to look more closely at augmented reality and its use in embodied learning. I really enjoyed reading the paper by Lindgren and Johnson-Glenberg (2013). This paper really emphasized the importance of “gestural congruency”, which is what sets embodied learning apart from hands-on activities or physical movement in general (Lindren & Johnson-Glenberg, 2013). Basically, the more congruent a physical gesture is to the learning concept, the higher the embodiment interaction. For example, when learning about centripetal force, a student who physically spins a trackable object overhead is participating in a high embodiment interaction in comparison to a student who just clicks on a mouse to initiate spinning in a computer based simulation. They argue that mixed reality (MR) environments are well suited for embodied learning because MR technology can create an immersive environment that situates students inside the to-be-learned environment. Additionally, it provides an environments with an interface that is responsive to students’ movements and physicality. They go on to state that educational researchers in the area of MR technology and embodied learning should focus on the following 6 strategies:
1) Ascribe to the benefits of body-based learning to everyone
- though there is learning variation to consider, they believe that this type of learning is beneficial to all types of learners, not just kinaesthetic ones. As such, the design of MR for education should be sensitive to cultural, physical and other types of differences among students
2) Assert action-concept congruencies
- They argue that to achieve educational goals, MR learning enivornmenst should be built upon substantiated links between physical actions that students perform and construction of new concepts (high embodiment interactions)
3) Augmentation should augur well
- I think their point on this one is that the MR tech should be used wisely and purposefully. Examples would be to overlay representational supports onto real-world experience, include unobservable phenomena, point out salient information, conduct multiple experiments in a short amount of time etc.
4) Introduce opportunities for collaborative implementation
5) Pair lab studies with real-world implementation
- They state that initial approach to studying a particular MR and learning would be to begin with controlled studies that examines specific affordances of MR tech from building conceptual knowledge before testing it in a authentic context (such as a school)
6) Re-envision assessment
- MR and embodied learning environments may have effects of learners’ intuition and understanding, perceptual acuity and their willingness to explore the domain but this may not be detected in traditional assessment methods. Thus the authors advocate for designing assessments that are more fit for this type of learning environment. They also state that delayed assessment is important
Now, keeping all of this in mind, I read a paper by Kamarainen et al (2013). This article explored utility of augmented reality paired with a handheld environmental probe to deliver an enhanced situated learning experience to students during a middle school ecosystem science field trip. The augmented reality portion was delivered through a mobile wireless device, which helped students navigate the pond environment and delivered virtual media and information overlaid on the physical pond. AR was also used to direct students to “hotspots” where they were instructed to use the environmental probe to collect measurements. There were several benefits of using AR with the environmental probe, which include:
- ability to provide contextualized, just-in-time instruction
- self-directed collection of real-world data and images
- social interactivity
- facilitate cognition distributed among people tools and context
- and provide individualized scaffolding
Their study found that students learned the intended content well according to a pre-and post activity content assessment, reported a high degree of self-efficacy and had a positive experience during the field trip.
However, I had several questions regarding this research study. For example, it’s hard to assess how much AR actually contributed to student content learning. Could something as low tech as a map and some written information been sufficient to produce the same effect? Is the content knowledge gained sustained? After the novelty of the new technology wears off, will engagement still be high? Was there some other way that AR could be used in a more high embodiment interaction? What is the cost (both for the program and time required to create the AR environment for a particular location) of creating such a program? Is it worth the cost? And could a teacher run a similar field trip without the tech support that was needed (2 researchers provided tech support during each field trip in addition to the one teacher and field trip coordinator that was also present)? I think AR provides a really intriguing field in education with a lot of potential but further research is needed.
Questions:
1. Have you come across any VR or AR environments for education that use high embodiment interactions?
2. In your opinion, are the costs of these VR or AR environments prohibitory to their use in education?
References
Kamarainen, A. M., Metcalf, S., Grotzer, T., Browne, A., Mazzuca, D., Tutwiler, M. S., & Dede, C. (2013). EcoMOBILE: Integrating augmented reality and probeware with environmental education field trips. Computers & Education, 68, 545–556. http://doi.org/10.1016/j.compedu.2013.02.018
Lindgren, R., & Johnson-Glenberg, M. (2013). Emboldened by Embodiment: Six Precepts for Research on Embodied Learning and Mixed Reality. Educational Researcher, 42(8), 445–452. http://doi.org/10.3102/0013189X13511661
A comparison of 4 TELEs
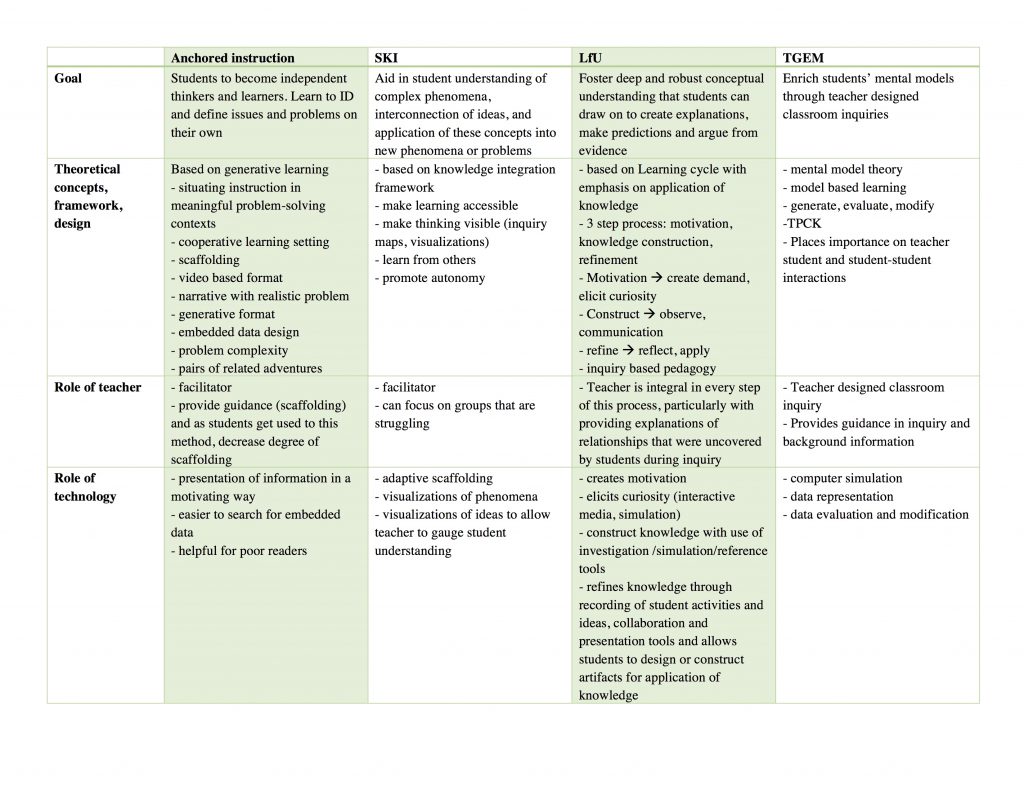
I decided to summarize the 4 TELEs in table format. This is what I came up with:
Below is a link to a PDF in case the above does not read well.
Module B synthesis
Synthesis
All methods noted in the table are based on constructivist learning theories. All methods aim to achieve a deeper understanding of complex phenomena or concept in math and/or science. I found that the use of technology for presentation of information was the same in each TELE, however, the degree to which technology was used for other things differed. For example, in the Jasper series (Anchored instruction), technology use was limited to presentation of information, whereas in WISE (SKI), MyWorld (LfU), and Chemland (T-GEM), it was also used for data evaluation, visualization of ideas and collaboration. The TELEs also differed in the degree of guidance or scaffolding that was provided as well as the provider of that scaffolding. For Jasper, the purpose was for generative learning, and thus minimal scaffolding would be provided (though this can be adjusted dependent on the preference of the teacher and experience of the students). In contrast, with MyWorld, the teacher provides guidance at each step and also provides explanations of relationships that were uncovered by students during the knowledge construction observation stage. In Jasper, MyWorld, and Chemland scaffolding was provided by the teacher. However in the WISE projects, much of the scaffolding was provided by technology in combination with the teacher particularly for those groups that were struggling.
T-GEM for cardiovascular physiology
A commonly cited conceptual challenge in medical education is cardiovascular physiology. This seems to be a consistent finding at different educational levels (Mikkila-Erdmann, 2012). If applying the T-GEM model (Khan, 2010)to teaching this, I would organize it as follows:
- I would provide some background content information, such as the definition of cardiac output, mean arterial pressure, heart rate, and systemic vascular resistance (total peripheral resistance)
- Have the students pair up and access the following simulator: https://ilearn.med.monash.edu.au/physiology/Cardiovascular/index.html
- on the Home tab, have the students look at the relationship between cardiac output, mean arterial pressure, and heart rate
- have students generate a relationship between the above variables (by seeing what happens to these variables during different activities)
- Based on this relationship, have students predict what will happen to these variables with postural change
- Have students run the postural change simulation and evaluate the relationship
- Have students review their initial predictions and compare to the relationship that was observed through the simulation.
- ask students to modify their initial predictions/relationships based on new data.
I think this method will offer students a chance to challenge their conceptual models by simulation and make modifications as needed. In trying to find software for TGEM in the medical context, I ran into a significant challenge. This is because a lot of medical simulations were for clinical skills or other technical skills improvement, and not for the purposes of understanding certain phenomena. But I do think this is a great way to learn and really understand concepts in a deeper more meaningful way (compared to the superficial rote memorization that is still common in medical education). I hope that simulations that examine concepts in my field become more readily available as time goes on.
References
Khan S. New Pedagogies on Teaching Science with Computer Simulations. J Sci Educ Technol. 2010;20(3):215-232. doi:10.1007/s10956-010-9247-2.
Mikkilä-Erdmann M, Södervik I, Vilppu H, Kääpä P, Olkinuora E. First-year medical students’ conceptual understanding of and resistance to conceptual change concerning the central cardiovascular system. Instr Sci. 2012;40(5):745-754. doi:10.1007/s11251-012-9212-y.
LfU – an application for pelvic anatomy?
According to Edelson (2001), LfU is based on 4 theories of learning, which are:
1) learning takes place through construction and modification of knowledge structures
2) knowledge construction is a goal-directed process, guided by a combination of conscious and unconscious understanding of goals
3) circumstances in which knowledge is constructed and subsequently used determine its accessibility for future use
4) knowledge must be constructed in a form that supports use before it is applied.
These principles underlie the LfU model, which is a three-step process involving
1) motivation
2) knowledge construction
3) knowledge refinement
In terms of technology, it plays many important roles within the LfU model. For example, it can play a role in eliciting curiosity (motivation), help students interactive with phenomena not possible in the real world which aids with knowledge construction and refinement.
So how would I apply it to a topic that I teach? The one thing that comes to mind is pelvic anatomy. Students tend to struggle with pelvic anatomy because it is quite complex and has multiple layers to it. I would start off by presenting students with a case of a patient who underwent surgery and shortly thereafter developed leg weakness and pain (this is actually one of the patient that presented to me early in my career). I would then have the students come up with theories based on their current knowledge level, regarding the cause of this pain/leg weakness. This is to draw their attention to their current level of knowledge and to have them recognize their limitations and thus increase motivation to learn. This would also create a context in their memory for integrating new knowledge (Edelson, 2001). Then I would use AnatomyTV, which is an interactive 3D anatomy resource (available through UBC at http://resources.library.ubc.ca/page.php?id=888) as my software of choice. This interactive resource that allows students to manipulate the body in 3D (select 3D Atlas —> Pelvis, then click female pelvis and perineum ~ tumble under 3D views from menu on the left to try it out!), which is really helpful, as most textbooks only present the learner with the upright position of the human body. This is not practical because in most gynecologic clinical practices, we examine patients and operate on them in the supine position, and thus knowledge of anatomy in this position is much more applicable. This program also allows the user to strip away all layers of the body and add them one by one, which allows students to understand how each layer relates to the other. I would also have student work in small group to promote interaction and discussion as this also aids in knowledge construction and refinement. Finally, I would have the students reflect on their initial theories, make any changes they feel are needed and present it as a group to the class and further apply their new knowledge to come up with a management plan for the patient. In this way, I believe I have applied the LfU principles to this topic.
References
1. Edelson DC. Learning‐for‐use: A framework for the design of technology‐supported inquiry activities. Journal of Research in Science Teaching. 2001;38(3):355-385. doi:10.1002/1098-2736
Space colony – a collaborative learning experience
I decided to look at the project “Space Colony! Genetic diversity and survival” (ID 175). In this project, the students are challenged to consider genetic mutations, diversity, and cloning as they decide how to colonize three different planets. I like this lesson as it challenges students to think about a variety to topics as they work through their challenge. Despite the number of topics, I believe it was presented in a very logical manner. What I thought was missing from this lesson was one of the tenets of SKI, which is learning from others (Linn, 2003). This component is something i really liked in some of the other projects that I viewed (such as the one on cystic fibrosis). So I built pages after the open ended questions to have students share their ideas/answers. Then a page on ideas/answers from others that they decided to copy (with explanations on why they wanted to copy them, or what about that idea really appealed to them) and finally a page that allows students to sort their ideas (both their own and from peers) and resubmit their answer to the original open ended question. I also had them reflect on whether or not their ideas changed and if so, for them to justify their changes. I felt that this addition promoted learning from others, as well as reflection on their own thoughts, and would support students as they actively constructed knowledge on these topics.
I felt this WISE project had all the other tenants of SKI (Linn, 2003), which are:
1. making learning accessible
2. making thinking visible
3. promote autonomy/life long learning
In regards to making learning accessible, despite talking about topics at the cellular and genetic level, they always tied to back to something students can relate to, such as siblings, twins, etc. They also brought in real life examples, such as “Dolly”, the first cloned sheep.
Throughout the lesson, they either asked open ended questions or multiple choice questions to gauge student understanding of concepts. This makes learning visible, increasing teacher awareness of students thoughts and diversity. They also incorporated a few simulations and great visuals to help students understand complex phenomena.
Finally, the project is organized in such a way that students learn the process of inquiry, which promotes autonomy in learning. I really liked the logical flow that this project has, and the final wrap up which brings all the concepts back together in the end. As such, I think I would run the project as it is presented, with just the added component of collaboration/learning from peers.
References
1. Linn MC, Clark D, Slotta JD. WISE design for knowledge integration. Science Education. 2003;87(4):517-538. doi:10.1002/sce.10086.
Jasper, anchored instruction and PBL
The theoretical framework that underpins the Jasper series is anchored instruction. Anchored instruction is instruction that is “situated in engaging, problem-rich environments that allow sustained exploration by students and teachers” (Cognition and Technology Group at Vanderbilt, 1992). The Jasper series is a video based instruction format that presents students with a complex problem, which requires many subproblems to be generated and solved for the main complex problem to be addressed. It uses an engaging narrative with embedded data to present the students with all the information they may require to engage with the complex problem. This instructional approach promotes several teaching and learning activities that are central to constructivism. This includes generative learning, collaboration, active learning and engagement, and construction of knowledge.
Certainly the Jasper series could be presented without the use of technology. However technology does enhance the teaching and learning activities mentioned above. For example, the use of video could make the material more engaging due to the increased realism afforded by the video format (though it is a little dated now). This notion is supported by several papers, as highlighted by Taylor and Parsons (2011) in their review of the literature on student engagement. It can also be helpful for those students with learning challenges where an audio only narrative or reading only narrative would present a significant barrier.
Medical education has certainly moved in this direction. During the first two years, we have increased exposure of students to real clinical environments where they would learn though clinical encounters in a situated learning environment. In addition to this, their didactic lectures are taught along side problem-based learning activities, which is essentially anchored instruction. Our school currently does not use a video format, but a written digital document is provided to students in small groups, which gives students a clinical scenario. They then discuss the case to figure out what is going on with the patient. In all groups, the members decide on what further knowledge is needed in order to move forward with the case scenario. During this discussion portion, they are not allowed to use any resources other than their own ideas and experiences, which promotes discussion, collaboration and reflection. Once they have established learning objectives for the group, the first session ends and they have 1-2 days to research their learning objectives (either collaboratively or individually, depending on the group). They then reconvene and discuss the learning objectives before more of the clinical scenario is revealed. Typically, each case is discussed over 2-3 group sessions.
I think that in our problem-based learning groups, technology can be used to enhance collaboration and generative learning. For example, concepts maps may be useful to organize the group’s thoughts in a visual manner, adding to collaboration and generation of ideas. The use of something like Google Docs which affords collaboration asynchronously could also be helpful in collaboration outside of the group meetings. A video format could also be helpful to refine students’ observational skills as this is a critical part of the medical assessment, and again help to create an authentic/realistic environment.
References
Cognition, Vanderbilt TGA. The Jasper experiment: An exploration of issues in learning and instructional design. ETR&D. 1992;40(1):65-80. doi:10.1007/BF02296707.
Taylor, L. & Parsons, J. (2011). Improving Student Engagement. Current Issues in Education,14(1). Retrieved from http://cie.asu.edu/
PCK/TPACK and the TVT
PCK/TPACK were definitely new terms for me. Though my idea of a “good” teacher was one who had both content knowledge and pedagogical knowledge specific to that content, I had never heard of it being described in such a concise manner. Looking at the many physicians that teach, particularly at the clinical level, they are definitely content experts with little or no pedagogical knowledge. Somehow it is presumed that having the content knowledge gives you the ability to teach medicine, which is far from the truth, and I have personally been on the receiving end of this. For example, experienced physicians are able to accomplish tasks in an “unconscious competent” manner. Looking at the diagram below, novice students and residents start at the “unconscious incompetent” stage of this cycle.
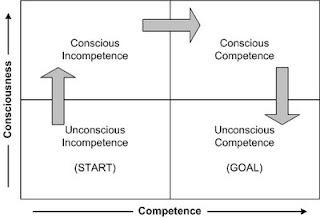
Adult learning cycle
They observe an expert accomplish something (such as suturing) and because the expert made it look so easy, presume that it can easily be accomplished. When they are given the opportunity to do the task themselves, they move into the “conscious incompetent” stage, where they begin to understand that it isn’t as easy as it looks and there are a lot of steps that they had not considered upon observation. With repeat practice, reflection, and learning with guidance, they enter the “conscious competent” stage, where they still have to think about each step but can complete the task competently. Clinical teachers facilitate their learners through this cycle, but because many of them are doing tasks in the “unconscious competent” state, sometimes they are unable to identify some of the steps that are automatic for them, and thus are missing the pedagogical knowledge component.
A common procedure that I perform that is difficult to learn is insertion of a device called a TVT. This device is used for the treatment of stress incontinence. It is difficult to learn because it is a relatively blind procedure, with a high bladder injury rate (which increases learner anxiety!) When teaching this procedure, I often break it down into several steps for my residents:
1) Observation – I will have them observe the procedure as I perform it. I will deliberately take my time performing each step, and explain each step as well as the rationale behind my movements.
2) Then I take them over to a pelvic model for simulation (after the observation). Again, I repeat the procedure, performing each step slowly and with explanation. I will also have them slide their hands over mine to feel where I am in relation to the anatomy (because most of it is done blindly).
3) Next, I have the learner verbally repeat the steps while visualizing
4) Then I have them perform the steps, verbalizing each step as perform it (on the model simulator).
5) I will have them repeat this on the model a few times until they are comfortable
6) At the next OR, if this procedure comes up, I will have them verbalized the steps with visualization prior to the case.
7) Finally, I will have them perform the case, while verbalizing each step, and provide guidance as needed. At this point, I gauge their level of comfort and competence and adjust my guidance as needed.
Over the last couple of years that I have been teaching this, I have modified the steps based on the areas that my learners seem to struggle the most. These areas are broken down into smaller steps, with simple instructions so the procedure is easier to understand and perform.